Hernández-Cruz Estefani Y, Aparicio-Trejo Omar E, Hammami Fadi A, Bar-Shalom Daniel, Tepel Martin, Pedraza-Chaverri Jose, Scholze Alexandra
Laboratory F-315, Department of Biology, Faculty of Chemistry, National Autonomous University of Mexico, Mexico City, Mexico.
Department of Cardio-Renal Pathophysiology, Ignacio Chávez National Institute of Cardiology, Mexico City, Mexico.
Kidney Int Rep. 2024 Jul 20;9(10):2883-2903. doi: 10.1016/j.ekir.2024.07.020. eCollection 2024 Oct.
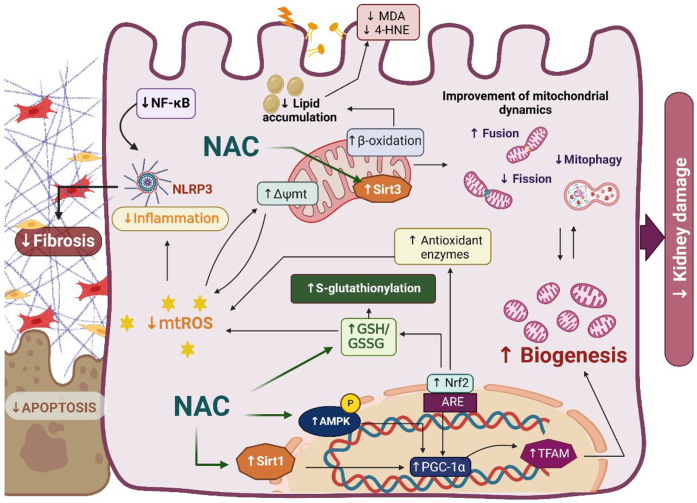
N-acetylcysteine (NAC) has shown beneficial effects in both acute kidney disease and chronic kidney disease (CKD) in preclinical and clinical studies. Different dosage and administration forms of NAC have specific pharmacokinetic properties that determine the temporal pattern of plasma concentrations of NAC and its active metabolites. Especially in acute situations with short-term NAC administration, appropriate NAC and glutathione (GSH) plasma concentrations should be timely ensured. For oral dosage forms, bioavailability needs to be established for the respective NAC formulation. Kidney function influences NAC pharmacokinetics, including a reduction of NAC clearance in advanced CKD. In addition, mechanisms of action underlying beneficial NAC effects depend on kidney function as well as comorbidities, both involving GSH deficiency, alterations in nuclear factor erythroid 2-related factor 2 (Nrf2)-dependent signaling, oxidative stress, mitochondrial dysfunction, and disturbed mitochondrial bioenergetics. This also applies to nonrenal NAC mechanisms. The timing of preventive NAC administration in relation to potential injury is important. NAC administration seems most effective either preceding, or preceding and paralleling conditions that induce tissue damage. Furthermore, studies suggest that very high concentrations of NAC should be avoided because they could exert reductive stress. Delayed administration of NAC might interfere with endogenous repair mechanisms. In conclusion, studies on NAC treatment regimens need to account for both NAC pharmacokinetics and NAC molecular effects. Kidney function of the patient population and pathomechanisms of the kidney disease should guide rational NAC trial design. A targeted trial approach and biomarker-guided protocols could pave the way for the use of NAC in precision medicine.
在临床前和临床研究中,N-乙酰半胱氨酸(NAC)已在急性肾损伤和慢性肾脏病(CKD)中显示出有益作用。NAC的不同剂量和给药形式具有特定的药代动力学特性,这些特性决定了NAC及其活性代谢产物血浆浓度的时间模式。特别是在短期给予NAC的急性情况下,应及时确保适当的NAC和谷胱甘肽(GSH)血浆浓度。对于口服剂型,需要确定各自NAC制剂的生物利用度。肾功能会影响NAC的药代动力学,包括晚期CKD中NAC清除率的降低。此外,NAC有益作用的潜在机制取决于肾功能以及合并症,两者均涉及GSH缺乏、核因子红细胞2相关因子2(Nrf2)依赖性信号传导改变、氧化应激、线粒体功能障碍和线粒体生物能量学紊乱。这也适用于非肾脏的NAC机制。预防性给予NAC相对于潜在损伤的时间很重要。NAC给药似乎在诱导组织损伤的情况之前、或之前并同时进行时最有效。此外,研究表明应避免使用非常高浓度的NAC,因为它们可能会产生还原应激。延迟给予NAC可能会干扰内源性修复机制。总之,关于NAC治疗方案的研究需要考虑NAC的药代动力学和分子效应。患者群体的肾功能和肾脏疾病的发病机制应指导合理的NAC试验设计。有针对性的试验方法和生物标志物引导的方案可为NAC在精准医学中的应用铺平道路。