From the Department of Neuroscience (W.Z.Y., A.V.D.W., H.B., V.G.J.), School of Translational Medicine, Monash University; Department of Neurology (W.Z.Y., A.V.D.W., O.G.S., H.B., V.G.J.), Alfred Health, Melbourne; Department of Neurology (O.G.S., K.B.), Box Hill Hospital; Department of Neurosciences (O.G.S., K.B.), Eastern Health Clinical School, Monash University, Box Hill; Neuroimmunology Centre (T.K.), Department of Neurology, Royal Melbourne Hospital; CORe (T.K.), Department of Medicine, University of Melbourne, Australia; Amiri Hospital (R.A.), Sharq, Kuwait; Perron Institute for Neurological and Translational Science (A.G.K., M.J.F.-P., W.M.C.), University of Western Australia, Nedlands; Centre for Molecular Medicine and Innovative Therapeutics (A.G.K., M.J.F.-P.), Murdoch University, Perth; Sir Charles Gairdner Hospital (A.G.K., W.M.C.), QEIIMC, Nedlands; University of Newcastle (J.L.-S.), Newcastle; Hunter New England Health (J.L.-S.), John Hunter Hospital, New South Wales, Australia; Karadeniz Technical University (C.B.), Medical Faculty, Trabzon; Izmir University of Economics (S.O.), Medical Point Hospital, Izmir, Turkey; University Hospital Center Zagreb (M.H.); University of Zagreb (M.H.), School of Medicine, Croatia; Monash Health (N.A.J.); Department of Medicine (N.A.J.), School of Clinical Sciences, Monash University, Melbourne, Australia; CHUM and Universite de Montreal (A.P., M.G., P.D.), Canada; Neurology Department (S.M.B.), Faculty of Medicine, Mazandaran University of Medical Sciences, Iran; University of New South Wales (Suzanne Hodgkinson), Sydney, Australia; Cliniques Universitaires Saint-Luc (V.V.P.), Brussels; Université Catholique de Louvain (V.V.P.); Universitary Hospital Ghent (G.L.); Department of Neurology (B.W.), Antwerp University Hospital, Edegem; Translational Neurosciences Research Group (B.W.), Faculty of Medicine and Health Sciences, University of Antwerp, Wilrijk, Belgium; CSSS Saint-Jérôme (J.P.), Saint-Jerome, Canada; Department of Neuroscience (M.F.), Neurology Unit-MS Center, S. Maria delle Croci Hospital, AUSL Romagna, Ravenna, Italy; Department of Biotechnological and Applied Clinical Sciences (M.F.), University of L'Aquila, Italy; Groene Hart Ziekenhuis (K.D.G.), Gouda, Netherlands; Charles University in Prague and General University Hospital (D.H., E.K.H.), Prague, Czech Republic; Yeditepe University Kosuyolu Hospital (R.K.), Neurological Sciences, Istanbul, Turkey; Department of Medical and Surgical Sciences and Advanced Technologies (F.P.), GF Ingrassia, Catania; UOS Sclerosi Multipla (F.P.), AOU Policlinico "G Rodloico-San Marco", University of Catania, Italy; University of Queensland (P.A.M.), Brisbane; Royal Brisbane and Women's Hospital (P.A.M.), Australia; Centro Sclerosi Multipla (D.M.), UOC Neurologia, Azienda Ospedaliera per l'Emergenza Cannizzaro, Catania, Italy; Koc University (A.A.), Istanbul, Turkey; Nemocnice Jihlava (Radek Ampapa), Jihlava, Czech Republic; Azienda Ospedaliera di Rilievo Nazionale San Giuseppe Moscati Avellino (D.S.), Avellino, Italy; Zuyderland Medical Center (O.H.H.G.), Sittard-Geleen; School for Mental Health and Neuroscience (O.H.H.G.), Maastricht University, The Netherlands; Centro Hospitalar Universitario de Sao Joao (M.J.S.); Faculty of Health Sciences (M.J.S.), University Fernando Pessoa, Porto, Portugal; Royal Victoria Hospital (Stella Hughes), Belfast, United Kingdom; Department of Neurology (R.G., S.M.), Research laboratory LR18SP03, Clinical investigation Center Neurosciences and Mental Health, Razi Hospital; Faculty of Medicine of Tunis (R.G., S.M.), University of Tunis El Manar, Tunis, Tunisia; Austin Health (R.A.M.), Melbourne, Australia; Haydarpasa Numune Training and Research Hospital (R.T.), Istanbul, Turkey; Azienda Sanitaria Unica Regionale Marche - AV3 (E.C.), Macerata, Italy; Sultan Qaboos University (A.A.-A.), Al-Khodh, Oman; Bakirkoy Education and Research Hospital for Psychiatric and Neurological Diseases (A.S.), Istanbul, Turkey; St. Michael's Hospital (J.O.), Toronto, Canada; and F. Hoffmann-La Roche Ltd (E.M.-L.R., S.G., N.P.), Basel, Switzerland.
Neurol Neuroimmunol Neuroinflamm. 2024 Nov;11(6):e200328. doi: 10.1212/NXI.0000000000200328. Epub 2024 Oct 23.
Women with multiple sclerosis (MS) are at risk of disease reactivation in the early postpartum period. Ocrelizumab (OCR) is an anti-CD20 therapy highly effective at reducing MS disease activity. Data remain limited regarding use of disease-modifying therapies (DMTs), including OCR, and disease activity during peripregnancy periods.
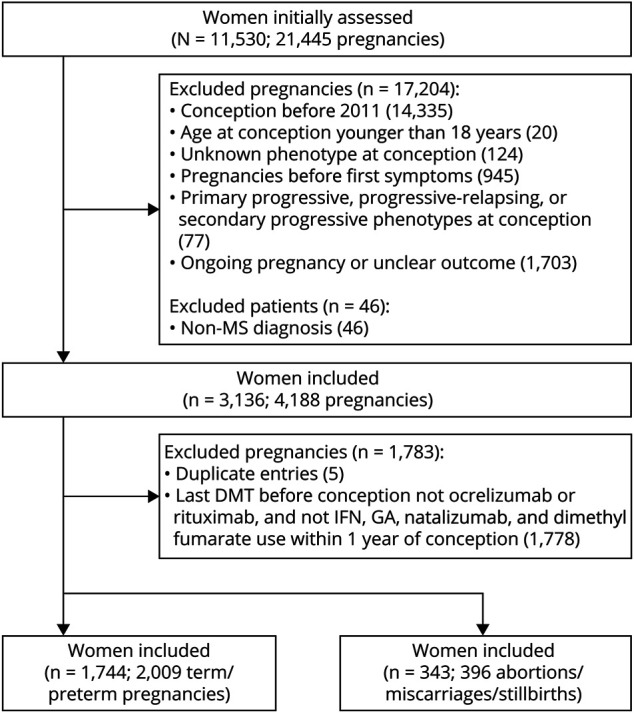
We performed a retrospective cohort study using data from the MSBase Registry including pregnancies conceived after December 31, 2010, from women aged 18 years and older, with relapsing-remitting MS or clinically isolated syndrome. Women were classified by preconception exposure to DMTs, including OCR, rituximab (RTX), natalizumab (NAT), stratified into active (NAT-A; continued ≥28 weeks of gestation, restarted ≤1 month postpartum) or conservative (NAT-C; continued ≤4 weeks of gestation, restarted >1 month postpartum) strategies, dimethyl fumarate (DMF) or low-efficacy DMTs (interferon-beta, glatiramer acetate). Annualized relapse rates (ARRs) were calculated for 12-month prepregnancy, pregnancy, and 6-month postpartum periods.
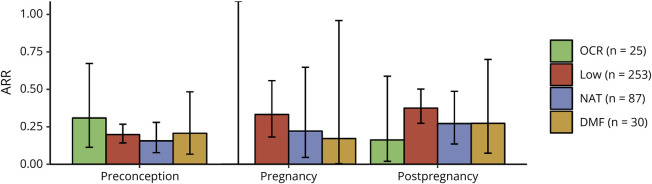
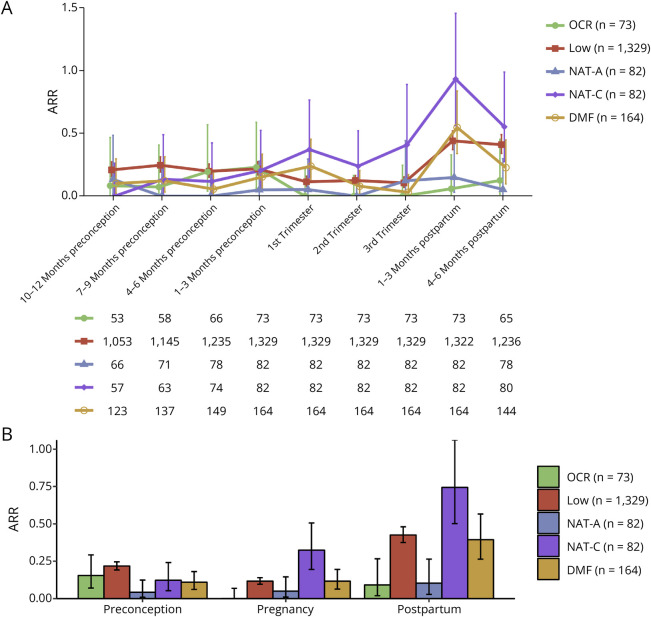
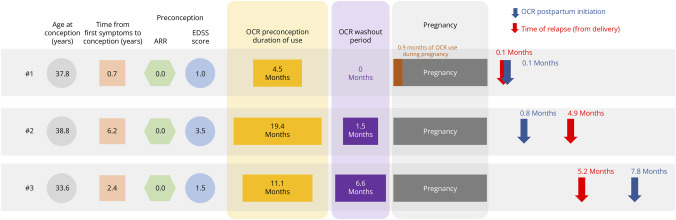
A total of 2,009 live births from 1,744 women were analyzed, including 73 live births from 69 women treated with preconception OCR. For OCR, no within-pregnancy relapse was observed and 3 women (4.1%) experienced 1 relapse in the postpartum period (ARR 0.09 [95% CI 0.02-0.27]). For NAT-A, 3 (3.7%) of 82 women relapsed during pregnancy (0.05 [0.01-0.15]) and 4 (4.9%) relapsed during postpartum (0.10 [0.03-0.26]). However, for NAT-C, 13 (15.9%) of 82 women relapsed within pregnancy (0.32 [0.20-0.51]) and 25 (30.5%) relapsed during postpartum (0.74 [0.50-1.06]). In the low-efficacy DMT group, 101 (7.6%) of 1,329 women experienced within-pregnancy relapse (0.12 [0.10-0.14]), followed by an increase in postpartum relapse activity with 234 women (17.6%) relapsing (0.43 [0.38-0.48]). This was similarly seen in the DMF group with 13 (7.9%) of 164 women experiencing within-pregnancy relapse (0.12 [0.06-0.20]) and 25 (15.2%) of 164 relapsing postpartum (0.39 [0.26-0.57]). Our RTX cohort had 0 of 24 women experiencing within-pregnancy relapse and 3 (12.5%) of 24 experiencing postpartum relapse.
Women treated with OCR or NAT-A were observed to have low relapse rates during pregnancy and postpartum. NAT-C was associated with increased risk of relapses. There was no within-pregnancy relapse in our RTX cohort, although we caution overinterpretation due to our sample size. An effective DMT strategy with a favorable safety profile for the mother and infant should be discussed and implemented well in advance of planning a family.
This study provides Class III evidence that for women with relapsing-remitting MS or clinically isolated syndrome who become pregnant, ocrelizumab, rituximab, and natalizumab (continued ≥28 weeks of gestation and restarted ≤1 month postpartum) were associated with reduced risk of relapses, compared with other therapeutic strategies.
患有多发性硬化症(MS)的女性在产后早期有疾病复发的风险。奥瑞珠单抗(OCR)是一种高效的抗 CD20 治疗药物,可有效降低 MS 疾病活动度。关于围孕期使用疾病修正疗法(DMT),包括 OCR,以及疾病活动度的数据仍然有限。
我们使用 MSBase 注册表中的数据进行了一项回顾性队列研究,其中包括 2010 年 12 月 31 日后受孕的年龄在 18 岁及以上、患有复发缓解型 MS 或临床孤立综合征的女性。根据女性在受孕前是否接触 DMT,包括 OCR、利妥昔单抗(RTX)、那他珠单抗(NAT),将女性分为积极(NAT-A;持续≥28 周妊娠,产后 1 个月内重新开始)或保守(NAT-C;持续≤4 周妊娠,产后 1 个月后重新开始)策略、二甲基富马酸(DMF)或低疗效 DMT(干扰素-β、格拉替雷)。计算了 12 个月孕前、妊娠和产后 6 个月的年化复发率(ARR)。
共分析了 1744 名女性的 2009 例活产,其中 69 名女性在受孕前接受 OCR 治疗,有 73 例活产。对于 OCR,未观察到妊娠期间复发,3 名女性(4.1%)在产后期间复发 1 次(ARR 0.09[95%CI 0.02-0.27])。对于 NAT-A,82 名女性中有 3 名(3.7%)在妊娠期间复发(0.05[0.01-0.15]),4 名(4.9%)在产后期间复发(0.10[0.03-0.26])。然而,对于 NAT-C,82 名女性中有 13 名(15.9%)在妊娠期间复发(0.32[0.20-0.51]),25 名(30.5%)在产后期间复发(0.74[0.50-1.06])。在低疗效 DMT 组中,1329 名女性中有 101 名(7.6%)在妊娠期间复发(0.12[0.10-0.14]),随后产后复发活动增加,234 名女性(17.6%)复发(0.43[0.38-0.48])。在 DMF 组中也观察到类似的情况,164 名女性中有 13 名(7.9%)在妊娠期间复发(0.12[0.06-0.20]),25 名(15.2%)在产后复发(0.39[0.26-0.57])。我们的 RTX 队列中,24 名女性中有 0 名在妊娠期间复发,3 名(12.5%)在产后复发。
接受 OCR 或 NAT-A 治疗的女性在妊娠和产后期间复发率较低。NAT-C 与复发风险增加相关。我们的 RTX 队列在妊娠期间没有复发,但由于我们的样本量较小,我们谨慎地避免过度解释。对于计划怀孕的女性,应该提前讨论并实施具有良好母亲和婴儿安全性的有效 DMT 策略。
这项研究提供了 III 级证据,对于患有复发缓解型 MS 或临床孤立综合征并怀孕的女性,与其他治疗策略相比,奥瑞珠单抗、利妥昔单抗和那他珠单抗(持续≥28 周妊娠,产后 1 个月内重新开始)与降低复发风险相关。