From the Department of Neurology (A.L.-G.), Los Angeles Medical Center, Southern California Permanente Medical Group; Departments of Clinical Science (A.L.-G.) and Health Systems Science (S.X.), Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena; Department of Research and Evaluation (B.H.L., J.B.S., S.X.), Southern California Permanente Medical Group, Pasadena, CA.
Neurol Neuroimmunol Neuroinflamm. 2024 May;11(3):e200211. doi: 10.1212/NXI.0000000000200211. Epub 2024 Mar 20.
B-cell-depleting therapies increase the risk of infections and hypogammaglobulinemia. These relationships are poorly understood. The objectives of these analyses were to estimate how much of this rituximab-associated infection risk is mediated by hypogammaglobulinemia and to identify other modifiable risk factors in persons with multiple sclerosis (pwMS).
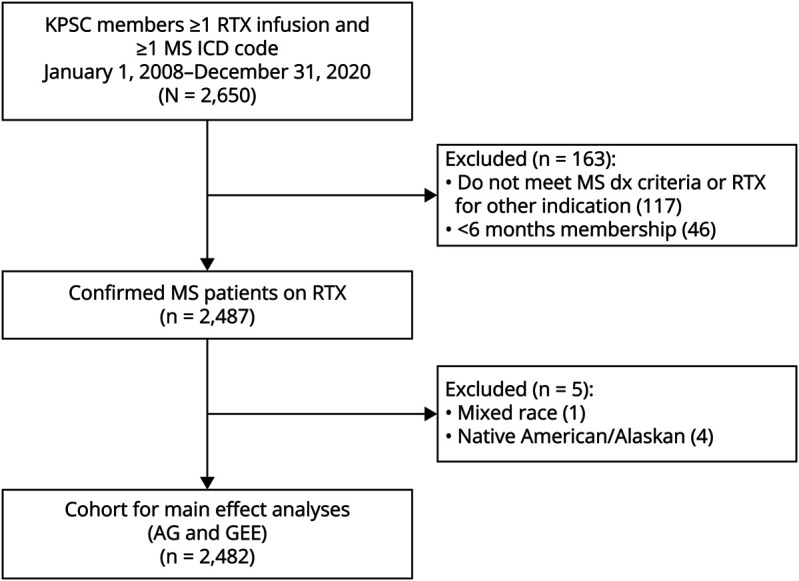
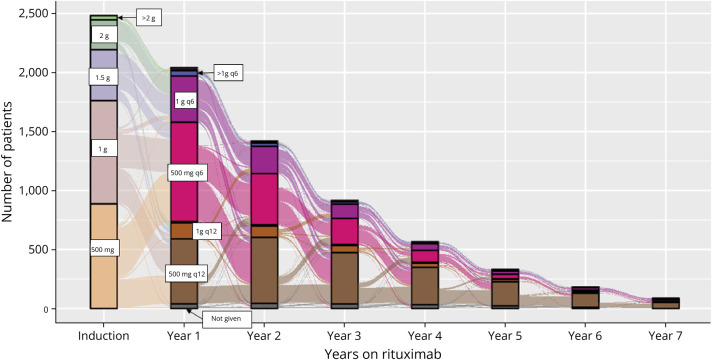
We conducted a retrospective cohort study of rituximab-treated pwMS from January 1, 2008, to December 31, 2020, in Kaiser Permanente Southern California. Cumulative rituximab dose was defined as ≤2, >2 and ≤4, or >4 g. Serious infections were defined as infections requiring or prolonging hospitalizations, and recurrent outpatient infections as seeking care for ≥3 within 12 months. Exposures, outcomes, and covariates were collected from the electronic health record. Adjusted hazard ratios (aHRs) were estimated using Andersen-Gill hazards models, and generalized estimating equations were used to examine correlates of IgG values. Cross-sectional causal mediation analyses of rituximab and hypogammaglobulinemia were conducted.
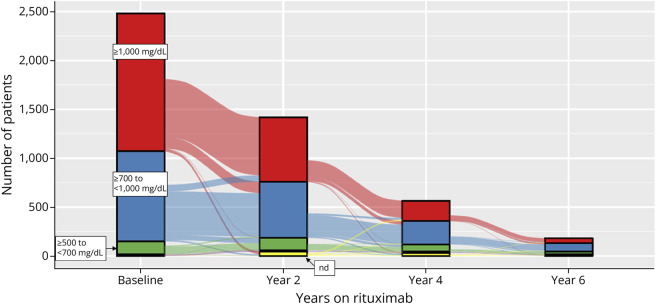
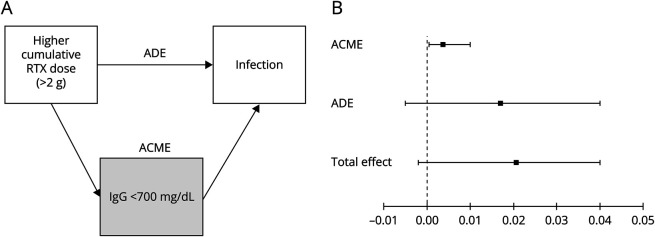
We identified 2,482 pwMS who were treated with rituximab for a median of 2.4 years (interquartile range = 1.3-3.9). The average age at rituximab initiation was 43.0 years, 71.9% were female, 49.7% were White, non-Hispanic patients, and 29.6% had advanced disability (requiring walker or worse). Seven hundred patients (28.2%) developed recurrent outpatient infections, 155 (6.2%) developed serious infections, and only 248 (10.0%) had immunoglobulin G (IgG) < 700 mg/dL. Higher cumulative rituximab dose (>4 g) was correlated with lower IgG levels (Beta = -58.8, < 0.0001, ref ≤2 g) and, in models mutually adjusted for hypogammaglobulinemia, both were independently associated with an increased risk of serious (>4 g, aHR = 1.56, 95% CI 1.09-2.24; IgG < 500, aHR = 2.98, 95% CI 1.56-5.72) and outpatient infections (>4 g, aHR = 1.73, 95% CI 1.44-2.06; IgG < 500 aHR = 2.06, 95% CI 1.52-2.80; ref = IgG ≥ 700). Hypogammaglobulinemia explained at most 17.9% (95% CI -47.2-119%) of serious infection risk associated with higher cumulative rituximab exposure but was not significant for outpatient infections. Other independent modifiable risk factors were advanced physical disability for serious (aHR = 5.51, 95% CI 3.71-8.18) and outpatient infections (aHR = 1.24, 95% CI 1.06-1.44) and COPD (aHR = 1.68, 95% CI 1.34-2.11) and obesity (aHR = 1.25, 95% CI 1.09-1.45) for outpatient infections.
Higher cumulative rituximab doses increase the risk of infections even in this population where 90% of patients maintained normal IgG levels. Clinicians should strive to use minimally effective doses of rituximab and other B-cell-depleting therapies and consider important comorbidities to minimize risks of infections.
B 细胞耗竭疗法会增加感染和低丙种球蛋白血症的风险。这些关系尚未得到充分理解。本分析的目的是估计利妥昔单抗相关感染风险中有多少是由低丙种球蛋白血症引起的,并确定多发性硬化症(MS)患者中的其他可改变的危险因素。
我们对 2008 年 1 月 1 日至 2020 年 12 月 31 日期间在 Kaiser Permanente Southern California 接受利妥昔单抗治疗的 MS 患者进行了回顾性队列研究。累积利妥昔单抗剂量定义为≤2、>2 和≤4 或>4 g。严重感染定义为需要或延长住院时间的感染,复发性门诊感染定义为在 12 个月内寻求≥3 次治疗的感染。从电子健康记录中收集暴露、结局和协变量。使用 Andersen-Gill 危害模型估计调整后的危害比(aHR),并使用广义估计方程检查 IgG 值的相关性。进行了利妥昔单抗和低丙种球蛋白血症的交叉因果中介分析。
我们确定了 2482 名接受利妥昔单抗治疗的 MS 患者,中位治疗时间为 2.4 年(四分位距=1.3-3.9)。利妥昔单抗起始年龄平均为 43.0 岁,71.9%为女性,49.7%为白人,非西班牙裔患者,29.6%有晚期残疾(需要助行器或更差)。700 名患者(28.2%)发生复发性门诊感染,155 名(6.2%)发生严重感染,只有 248 名(10.0%)免疫球蛋白 G(IgG)<700 mg/dL。较高的累积利妥昔单抗剂量(>4 g)与较低的 IgG 水平相关(Beta=-58.8,<0.0001,参考≤2 g),并且在相互调整低丙种球蛋白血症的模型中,两者均与严重感染(>4 g,aHR=1.56,95%CI 1.09-2.24;IgG<500,aHR=2.98,95%CI 1.56-5.72)和门诊感染(>4 g,aHR=1.73,95%CI 1.44-2.06;IgG<500,aHR=2.06,95%CI 1.52-2.80;参考 IgG≥700)的风险增加独立相关。低丙种球蛋白血症最多解释了与较高累积利妥昔单抗暴露相关的严重感染风险的 17.9%(95%CI-47.2-119%),但对门诊感染无统计学意义。其他独立的可改变危险因素是晚期身体残疾与严重感染(aHR=5.51,95%CI 3.71-8.18)和门诊感染(aHR=1.24,95%CI 1.06-1.44)以及 COPD(aHR=1.68,95%CI 1.34-2.11)和肥胖(aHR=1.25,95%CI 1.09-1.45)与门诊感染。
即使在 90%的患者保持正常 IgG 水平的情况下,较高的累积利妥昔单抗剂量也会增加感染的风险。临床医生应努力使用最小有效剂量的利妥昔单抗和其他 B 细胞耗竭疗法,并考虑重要的合并症,以最大限度地降低感染风险。