Akpa Bimaje, Pusalavidyasagar Snigdha, Iber Conrad
Division of Pulmonary, Critical Care & Sleep Medicine, University of Minnesota Medical School, Minneapolis, MN, USA.
J Thorac Dis. 2024 Sep 30;16(9):6292-6307. doi: 10.21037/jtd-23-1931. Epub 2024 Sep 26.
Respiratory care is often embedded as a component of the overlapping management strategies in many patients with neuromuscular disease (NMD). Implementation of respiratory care strategies requires a sensitivity to the nature of the disease, the vulnerability during rapid eye movement (REM) sleep and complicating comorbidities specific to each patient. Care must adjust to progression of the disease as well as the comfort and preferences of the patient. Clinical presentations are usually heterogenous based on the specific NMD and overall course of the disease making diagnosis and respiratory care challenging. The aim of this review was to review the state-of-the-art evidence-based clinical practices and updates in the management of respiratory complications in patients with NMDs.
We conducted a search on the PubMed and Medline databases using these keywords: secretions, neuromuscular disease, neuromuscular disorders, non-invasive ventilator, neuromuscular respiratory weakness, respiratory failure. The specified timeframe began from 1980 to 2024.
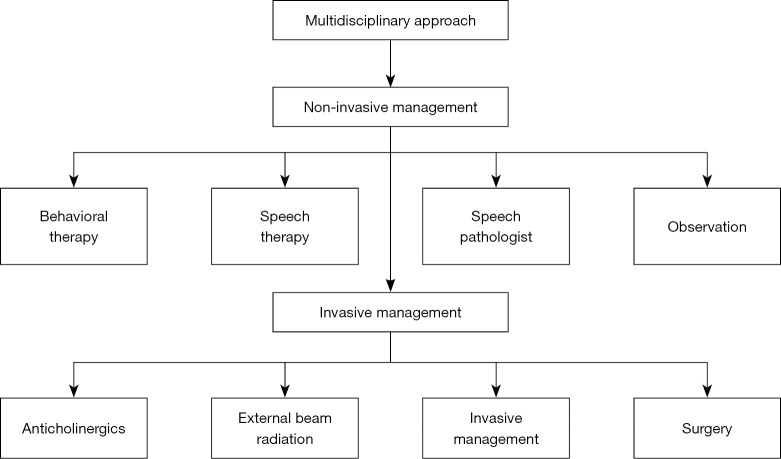
Timely use of non-invasive ventilation and overall respiratory care is most important as emerging evidence shows some benefits with improved mortality in this group of patients. In some settings, comorbid complications that dictate need for airway management and oral diversion may have a more profound impact on mortality than the effectiveness of ventilatory support that are chosen. A multidisciplinary team approach to care has been shown to improve the quality of life and survival in these patients in centers of excellence. Patients should have the ability to access services provided by neurology, pulmonology, speech pathology, sleep medicine, cardiology and respiratory therapy services.
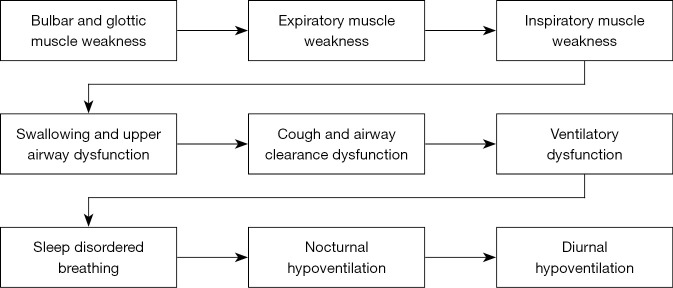
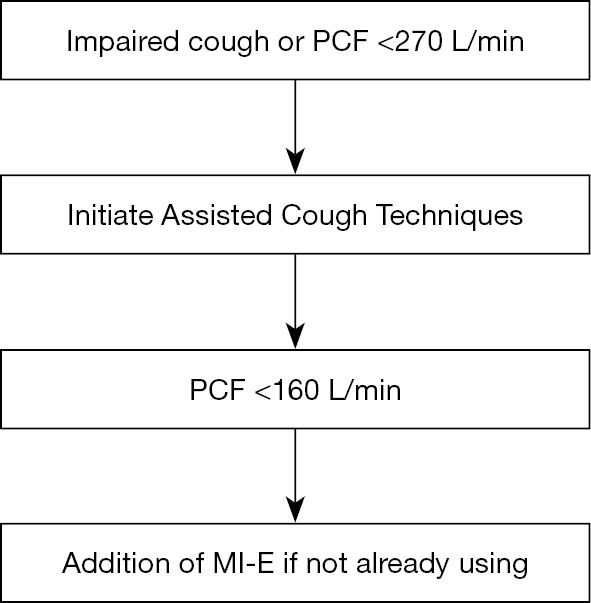
The cornerstone for management of respiratory failure and sleep disordered breathing in NMD is non-invasive ventilation (NIV). Initiation of this support and other respiratory cares need to be timely, and patients may have very subtle symptoms during the early stages of the disease which makes it challenging in recognizing the onset of respiratory muscle stress and fatigue. Close attention to these symptoms as well as respiratory and radiologic parameters is essential for appropriate incorporation of these cares.
在许多神经肌肉疾病(NMD)患者中,呼吸护理常常是重叠管理策略的一个组成部分。实施呼吸护理策略需要对疾病的性质、快速眼动(REM)睡眠期间的易损性以及每个患者特有的复杂合并症保持敏感。护理必须根据疾病的进展以及患者的舒适度和偏好进行调整。基于特定的神经肌肉疾病和疾病的整体病程,临床表现通常是异质性的,这使得诊断和呼吸护理具有挑战性。本综述的目的是回顾神经肌肉疾病患者呼吸并发症管理的最新循证临床实践和进展。
我们使用以下关键词在PubMed和Medline数据库中进行了检索:分泌物、神经肌肉疾病、神经肌肉障碍、无创通气、神经肌肉呼吸肌无力、呼吸衰竭。指定的时间范围从1980年至2024年。
及时使用无创通气和全面的呼吸护理最为重要,因为新出现的证据表明,这对改善该组患者的死亡率有一些益处。在某些情况下,决定气道管理和口腔引流需求的合并症可能比所选择的通气支持效果对死亡率有更深远的影响。在卓越中心,多学科团队护理方法已被证明可改善这些患者的生活质量和生存率。患者应能够获得神经病学、肺病学、言语病理学、睡眠医学、心脏病学和呼吸治疗服务提供的服务。
神经肌肉疾病中呼吸衰竭和睡眠呼吸障碍管理的基石是无创通气(NIV)。启动这种支持和其他呼吸护理需要及时,并且患者在疾病早期可能有非常细微的症状,这使得识别呼吸肌应激和疲劳的发作具有挑战性。密切关注这些症状以及呼吸和放射学参数对于适当纳入这些护理至关重要。