Öztürk N Begüm, Dadamyan Artem, Jamil Laith H
Department of Internal Medicine, Corewell Health William Beaumont University Hospital, Royal Oak, MI 48073, USA.
Oakland University William Beaumont School of Medicine, Rochester, MI 48309, USA.
Healthcare (Basel). 2024 Oct 21;12(20):2091. doi: 10.3390/healthcare12202091.
Gallbladder cancer (GBC) is a rare and aggressive hepatobiliary malignancy with poor prognosis. The symptoms of GBC are insidious and non-specific in its early stages, and most patients are diagnosed at advanced or late stages. Surgical resection is the only potentially curative treatment for GBC for select patients. There is a lack of robust data for patients with GBC, leading to heterogenous practices in management strategies and outcomes. In this study, we aimed to identify patient characteristics and cumulative overall survival (OS) in patients with GBC who underwent surgical resection with curative intent.
All adult patients (age ≥18 years) with localized or locoregionally advanced GBC who underwent definitive surgery with curative intent at our tertiary institution between 1/2013 and 12/2023 were retrospectively identified. Clinical, laboratory, radiology, histopathology, treatment, and survival data were collected from electronic medical records. Postoperative data included the use of adjuvant chemotherapy or radiotherapy, and patient survival mortality at a cut-off date of 1 February, 2024, calculated from the date of curative surgery. Continuous variables are reported as median and quartile 1 (Q1) and quartile 3 (Q3), while categorical variables are reported as counts and percentages.
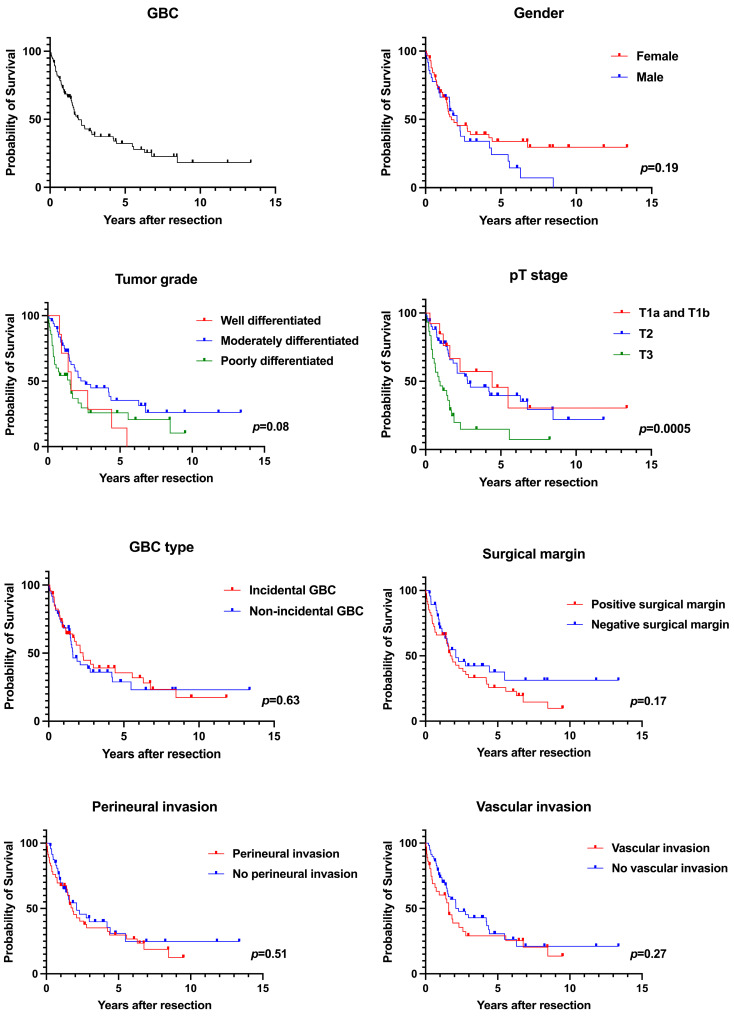
A total of 94 patients with GBC were included in the study. Median age was 71 (62-77) years and 58 (61.7%) patients were female. Median tumor size was 3.3 (1.9-5.0) cm. Perineural invasion was seen in 48.9% and vascular invasion in 38.3% of patients. A positive surgical margin was present in 50% of the patients, and incidental GBC (IGBC) was seen in 48.9% of patients. Tumor grade was well differentiated in 7.6%, moderately differentiated in 53.3%, and poorly differentiated in 39.1% of the patients. Patients with stage T1a (2.1%) and T1b (11.7%) tumors comprised the minority, and the majority of the tumors were stage T2 (55.3%), followed by T3 (31.9%). A total of 60.6% of patients with GBC underwent adjuvant chemotherapy, and 17% underwent adjuvant radiotherapy after surgical resection. Overall, 62 (66.0%) patients died, and the median OS was 1.88 years. The 1-year OS was 68.7%, 3-year OS was 37.4%, and 5-year OS was 32.2%. A higher absolute median OS was seen in patients who had adjuvant chemotherapy (2.1 years) compared to no chemotherapy (1.9 years); however, this finding was not statistically significant ( = 0.36). The median survival was 2.3 years in IGBC compared to 1.6 years in non-IGBC ( = 0.63).
GBC is an aggressive hepatobiliary malignancy that is often diagnosed at advanced stages. Our study showed high rates of local and systemic involvement and high mortality, and the need for prospective and randomized studies on adjuvant therapies to assess their survival benefit. Real-world patient data remain important to identify patients at risk of worse outcomes and to stratify risks prior to surgery.
胆囊癌(GBC)是一种罕见且侵袭性强的肝胆恶性肿瘤,预后较差。GBC在早期阶段症状隐匿且不具特异性,大多数患者在晚期或终末期才被诊断出来。手术切除是部分GBC患者唯一可能治愈的治疗方法。目前缺乏关于GBC患者的可靠数据,导致管理策略和治疗结果存在差异。在本研究中,我们旨在确定接受根治性手术切除的GBC患者的特征和累积总生存期(OS)。
回顾性纳入2013年1月至2023年12月期间在我们的三级医疗机构接受根治性手术的所有成年(年龄≥18岁)局限性或局部区域晚期GBC患者。从电子病历中收集临床、实验室、放射学、组织病理学、治疗和生存数据。术后数据包括辅助化疗或放疗的使用情况,以及截至2024年2月1日的患者生存死亡率,从根治性手术日期开始计算。连续变量以中位数和四分位数1(Q1)及四分位数3(Q3)报告,分类变量以计数和百分比报告。
本研究共纳入94例GBC患者。中位年龄为71(62 - 77)岁,58例(61.7%)为女性。中位肿瘤大小为3.3(1.9 - 5.0)cm。48.9%的患者出现神经周围侵犯,38.3%的患者出现血管侵犯。50%的患者手术切缘阳性,48.9%的患者为意外胆囊癌(IGBC)。7.6%的患者肿瘤分级为高分化,53.3%为中分化,39.1%为低分化。T1a期(2.1%)和T1b期(11.7%)肿瘤患者占少数,大多数肿瘤为T2期(55.3%),其次是T3期(31.9%)。共有60.6%的GBC患者接受了辅助化疗,17%的患者在手术切除后接受了辅助放疗。总体而言,62例(66.0%)患者死亡,中位OS为1.88年。1年OS为68.7%,3年OS为37.4%,5年OS为32.2%。接受辅助化疗的患者中位OS绝对值(2.1年)高于未接受化疗的患者(1.9年);然而,这一发现无统计学意义(P = 0.36)。IGBC患者的中位生存期为2.3年,而非IGBC患者为1.6年(P = 0.63)。
GBC是一种侵袭性强的肝胆恶性肿瘤,常于晚期被诊断出来。我们的研究显示局部和全身受累率高、死亡率高,且需要进行前瞻性随机研究以评估辅助治疗的生存获益。真实世界的患者数据对于识别预后较差风险的患者以及在手术前进行风险分层仍然很重要。