Dall'Ara Gianni, Piciucchi Sara, Carletti Roberto, Vizzuso Antonio, Gardini Elisa, De Vita Maria, Dallaserra Chiara, Campacci Federica, Di Giannuario Giovanna, Grosseto Daniele, Rinaldi Giovanni, Vecchio Sabine, Mantero Federica, Mellini Lorenzo, Albini Alessandra, Giampalma Emanuela, Poletti Venerino, Galvani Marcello
Cardiology Unit, Morgagni-Pierantoni Hospital, 47121 Forlì, Italy.
Department of Medical and Surgical Sciences (DIMEC), University of Bologna, 47121 Forlì, Italy.
J Cardiovasc Dev Dis. 2024 Oct 11;11(10):319. doi: 10.3390/jcdd11100319.
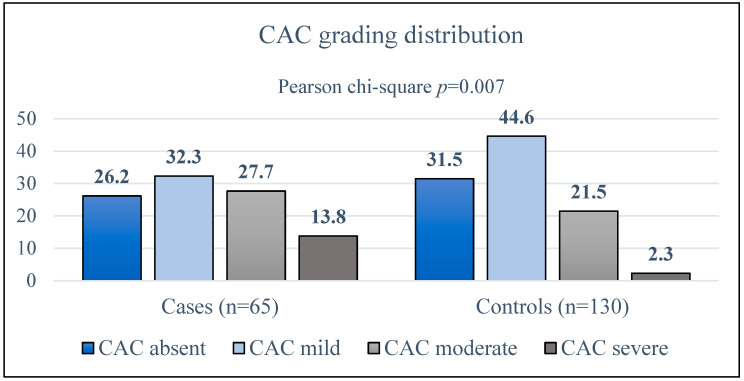
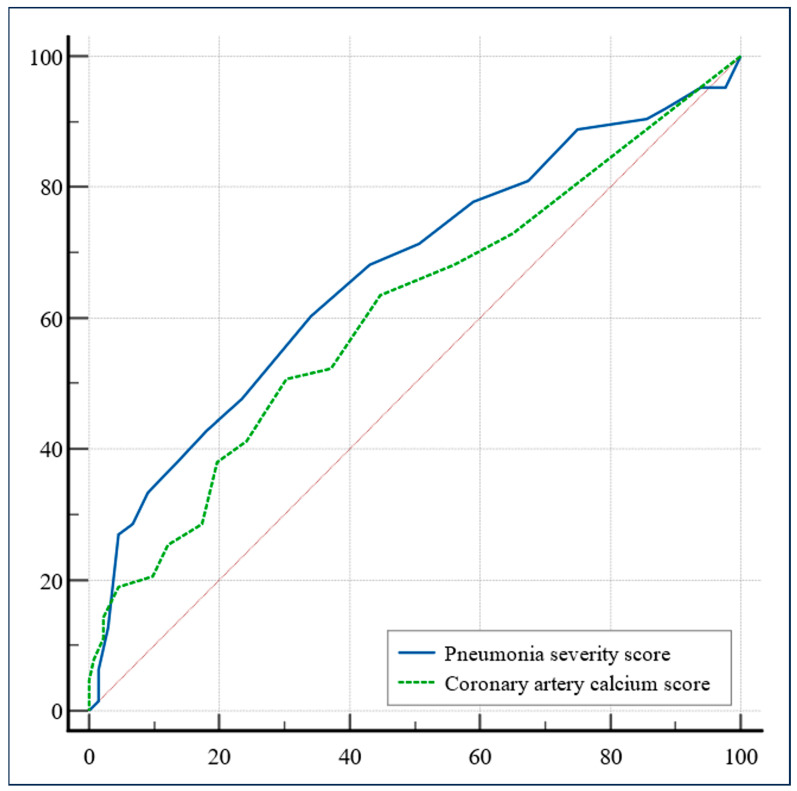
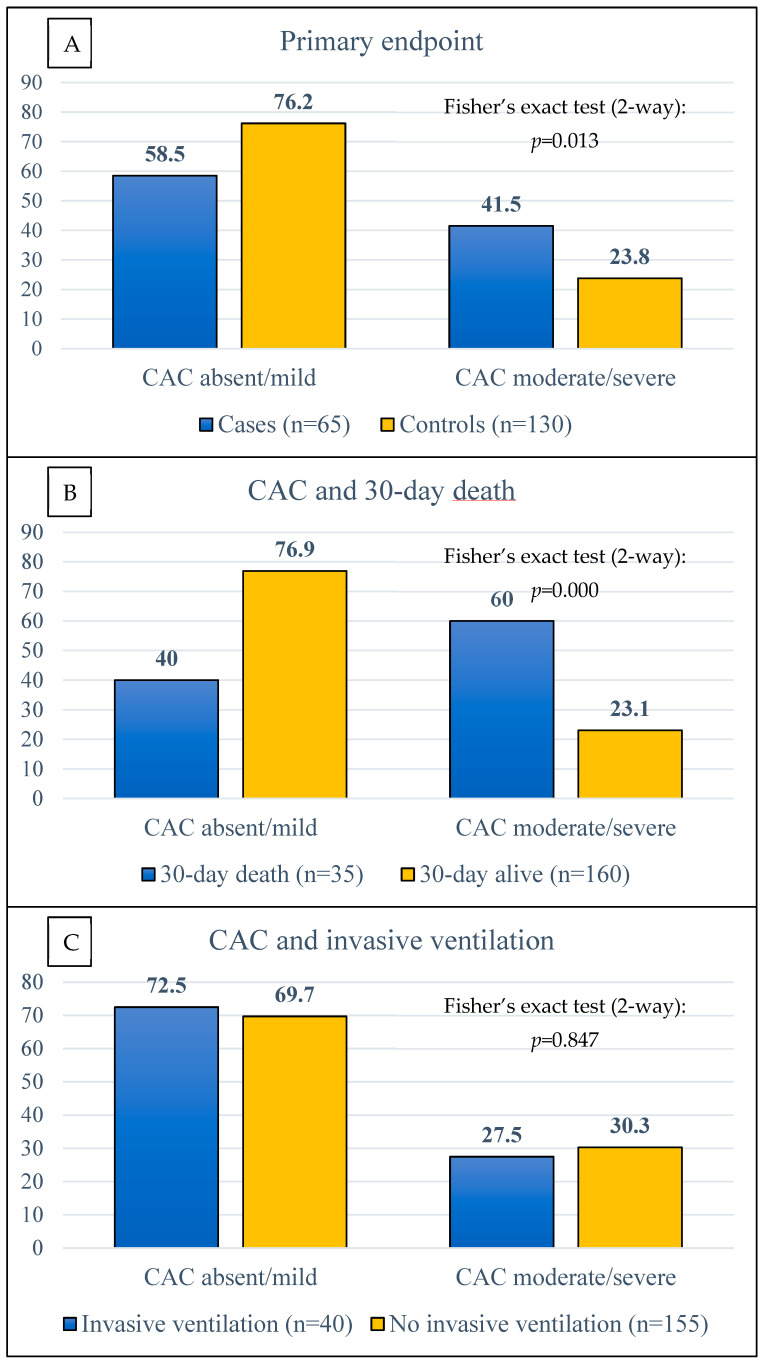
Patients suffering from coronavirus disease-19 (COVID-19)-related interstitial pneumonia have variable outcomes, and the risk factors for a more severe course have yet to be comprehensively identified. Cohort studies have suggested that coronary artery calcium (CAC), as estimated at chest computed tomography (CT) scan, correlated with patient outcomes. However, given that the prevalence of CAC is gender- and age-dependent, the influence of baseline confounders cannot be completely excluded. We designed a retrospective, multicenter case-control study including patients with COVID-19, with severe course cases selected based on death within 30 days or requiring invasive ventilation, whereas controls were age- and sex-matched patients surviving up to 30 days without invasive ventilation. The primary outcome was the analysis of moderate-to-severe CAC prevalence between cases and controls. A total of 65 cases and 130 controls were included in the study. Cases had a significantly higher median pulmonary severity score at chest CT scan compared to controls (10 vs. 8, respectively; = 0.0001), as well as a higher CAC score (5 vs. 2; = 0.009). The prevalence of moderate-to-severe CAC in cases was significantly greater (41.5% vs. 23.8%; = 0.013), a difference mainly driven by a higher prevalence in those who died within 30 days ( = 0.000), rather than those requiring invasive ventilation ( = 0.847). White blood cell count, moderate-to-severe CAC, the need for antibiotic therapy, and severe pneumonia at CT scan were independent primary endpoint predictors. This case-control study demonstrated that the CAC burden was higher in COVID-19 patients who did not survive 30 days or who required mechanical ventilation, and CAC played an independent prognostic role.
患有新型冠状病毒肺炎(COVID-19)相关间质性肺炎的患者预后各不相同,而病情更严重的危险因素尚未得到全面识别。队列研究表明,胸部计算机断层扫描(CT)估算的冠状动脉钙化(CAC)与患者预后相关。然而,鉴于CAC的患病率与性别和年龄有关,基线混杂因素的影响不能完全排除。我们设计了一项回顾性、多中心病例对照研究,纳入COVID-19患者,严重病例根据30天内死亡或需要有创通气来选择,而对照组为年龄和性别匹配、存活30天且无需有创通气的患者。主要结局是分析病例组和对照组中中重度CAC的患病率。该研究共纳入65例病例和130例对照。与对照组相比,病例组胸部CT扫描时的中位肺部严重程度评分显著更高(分别为10和8;P = 0.0001),CAC评分也更高(5和2;P = 0.009)。病例组中重度CAC的患病率显著更高(41.5%对23.8%;P = 0.013),这种差异主要由30天内死亡者的较高患病率所致(P = 0.000),而非需要有创通气者(P = 0.847)。白细胞计数、中重度CAC、抗生素治疗需求以及CT扫描显示的重症肺炎是独立的主要终点预测因素。这项病例对照研究表明,在未存活30天或需要机械通气的COVID-19患者中,CAC负担更高,且CAC发挥了独立的预后作用。