Institute for Systems Biology, Seattle, WA, USA.
Molecular Engineering & Sciences Institute, University of Washington, Seattle, WA, USA.
BMC Med. 2024 Oct 25;22(1):495. doi: 10.1186/s12916-024-03717-0.
Pregnant women are significantly underrepresented in clinical trials, yet most of them take medication during pregnancy despite the limited safety data. The objective of this study was to characterize medication use during pregnancy and apply propensity score matching method at scale on patient records to accelerate and prioritize the drug effect signal detection associated with the risk of preterm birth and other adverse pregnancy outcomes.
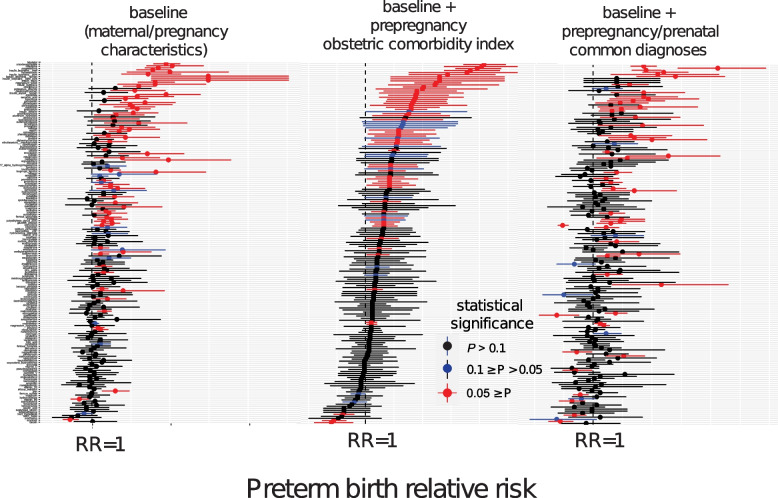
This was a retrospective study on continuously enrolled women who delivered live births between 2013/01/01 and 2022/12/31 (n = 365,075) at Providence St. Joseph Health. Our exposures of interest were all outpatient medications prescribed during pregnancy. We limited our analyses to medication that met the minimal sample size (n = 600). The primary outcome of interest was preterm birth. Secondary outcomes of interest were small for gestational age and low birth weight. We used propensity score matching at scale to evaluate the risk of these adverse pregnancy outcomes associated with drug exposure after adjusting for demographics, pregnancy characteristics, and comorbidities.
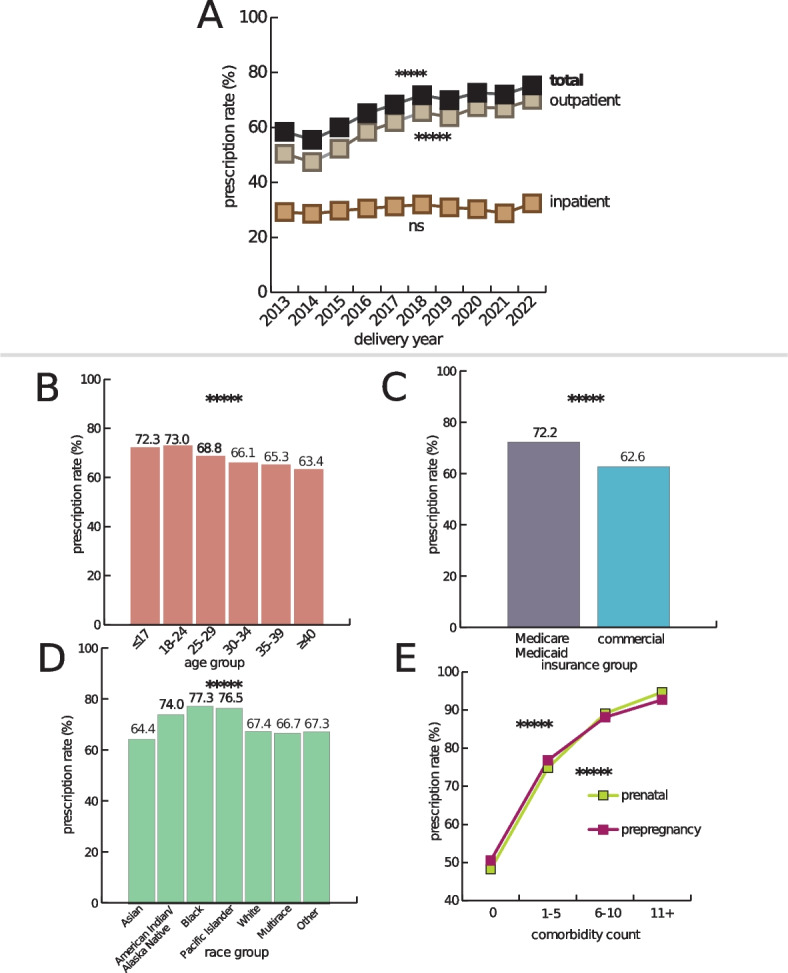
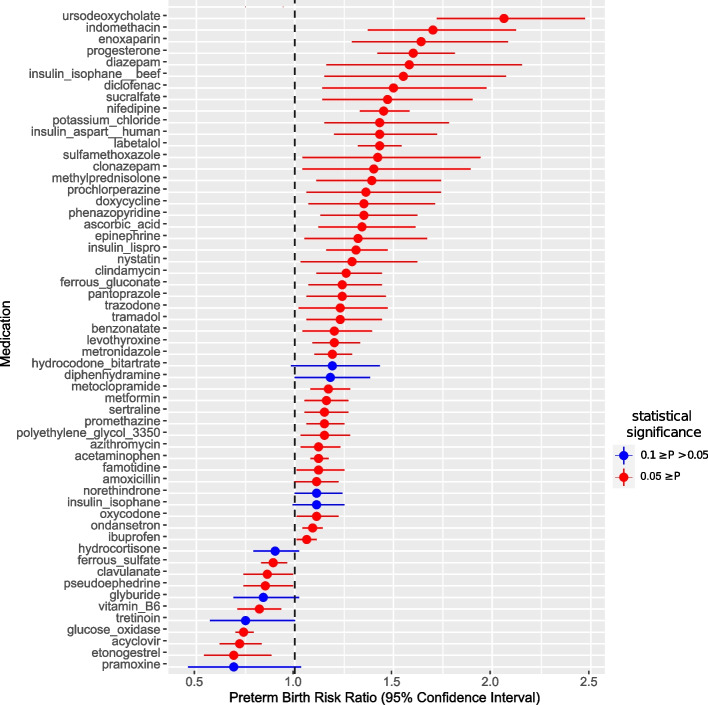
The total medication prescription rate increased from 58.5 to 75.3% (P < 0.0001) from 2013 to 2022. The prevalence rate of preterm birth was 7.7%. One hundred seventy-five out of 1329 prenatally prescribed outpatient medications met the minimum sample size. We identified 58 medications statistically significantly associated with the risk of preterm birth (P ≤ 0.1; decreased: 12, increased: 46).
Most pregnant women are prescribed medication during pregnancy. This highlights the need to utilize existing real-world data to enhance our knowledge of the safety of medications in pregnancy. We narrowed down from 1329 to 58 medications that showed statistically significant association with the risk of preterm birth even after addressing numerous covariates through propensity score matching. This data-driven approach demonstrated that multiple testable hypotheses in pregnancy pharmacology can be prioritized at scale and lays the foundation for application in other pregnancy outcomes.
尽管关于药物安全性的数据有限,但大多数孕妇在怀孕期间仍会服用药物,但临床试验中孕妇的代表性严重不足。本研究的目的是描述孕妇在怀孕期间的用药情况,并应用倾向评分匹配方法对患者记录进行大规模分析,以加速和优先检测与早产和其他不良妊娠结局风险相关的药物效应信号。
这是一项回顾性研究,纳入了 2013 年 1 月 1 日至 2022 年 12 月 31 日期间在普罗维登斯圣约瑟夫健康中心分娩的连续入组孕妇(n=365075)。我们感兴趣的暴露因素是所有在怀孕期间开具的门诊药物。我们将分析仅限于符合最小样本量要求的药物(n=600)。主要研究结果是早产。次要研究结果是胎儿生长受限和低出生体重。我们使用倾向评分匹配方法对药物暴露与这些不良妊娠结局风险之间的关系进行了大规模评估,调整了人口统计学、妊娠特征和合并症等因素。
总的药物处方率从 2013 年的 58.5%增加到 2022 年的 75.3%(P<0.0001)。早产的发生率为 7.7%。在 1329 种产前开具的门诊药物中,有 175 种符合最小样本量要求。我们确定了 58 种药物与早产风险有统计学显著关联(P≤0.1;减少:12,增加:46)。
大多数孕妇在怀孕期间会服用药物。这突出表明需要利用现有真实世界数据来增强我们对妊娠期间药物安全性的认识。即使在通过倾向评分匹配处理了多个协变量后,我们将从 1329 种药物缩小到 58 种与早产风险有统计学显著关联的药物。这种数据驱动的方法表明,可以大规模优先考虑妊娠药理学中的多个可检验假设,并为其他妊娠结局的应用奠定基础。