Chedid El Helou Michel, Gupta Mohak, Hussain Muzna, Hanna Mazen, Blumer Vanessa, William Preethi, Desai Milind Y, Abadie Bryan Q, Ives Lauren, Tang W H Wilson, Jaber Wael A, Collier Patrick, Martyn Trejeeve
Department of Cardiovascular Imaging, Heart, Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, OH 44195, USA.
Department of Internal Medicine, Cleveland Clinic, Cleveland, OH 44195, USA.
J Clin Med. 2024 Oct 16;13(20):6150. doi: 10.3390/jcm13206150.
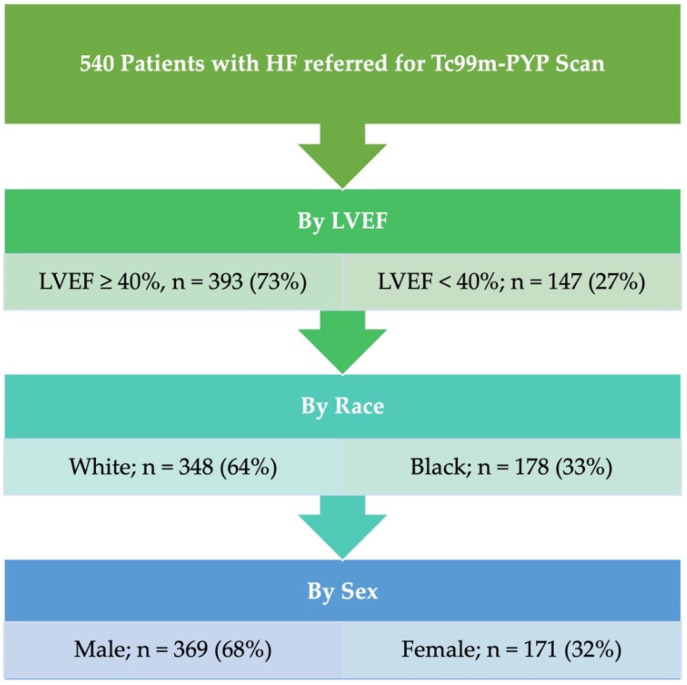
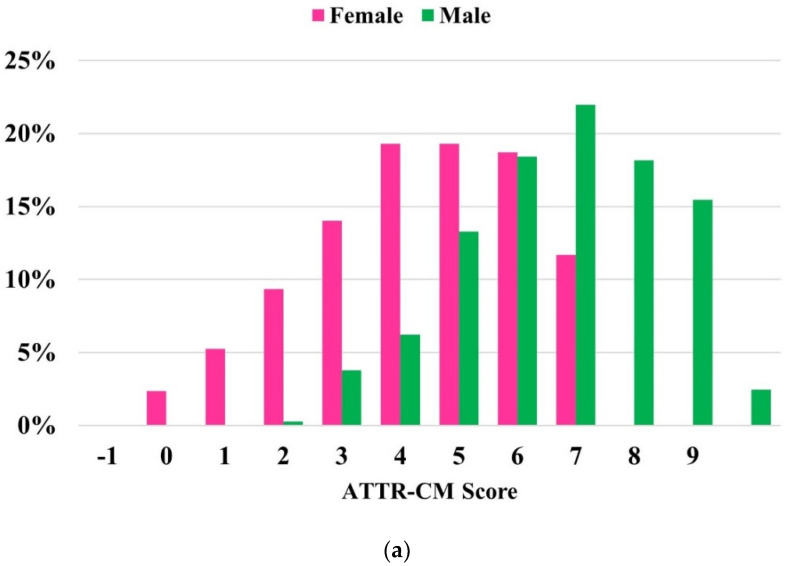
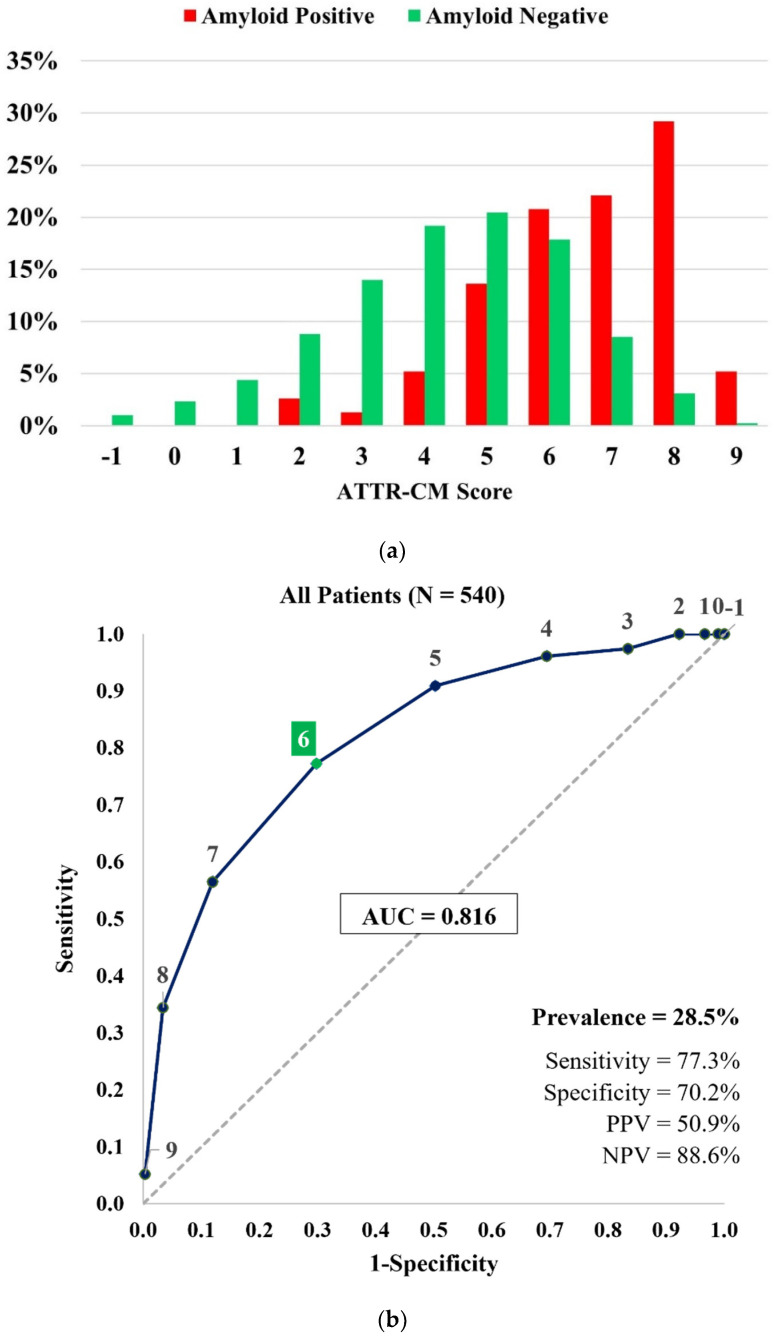
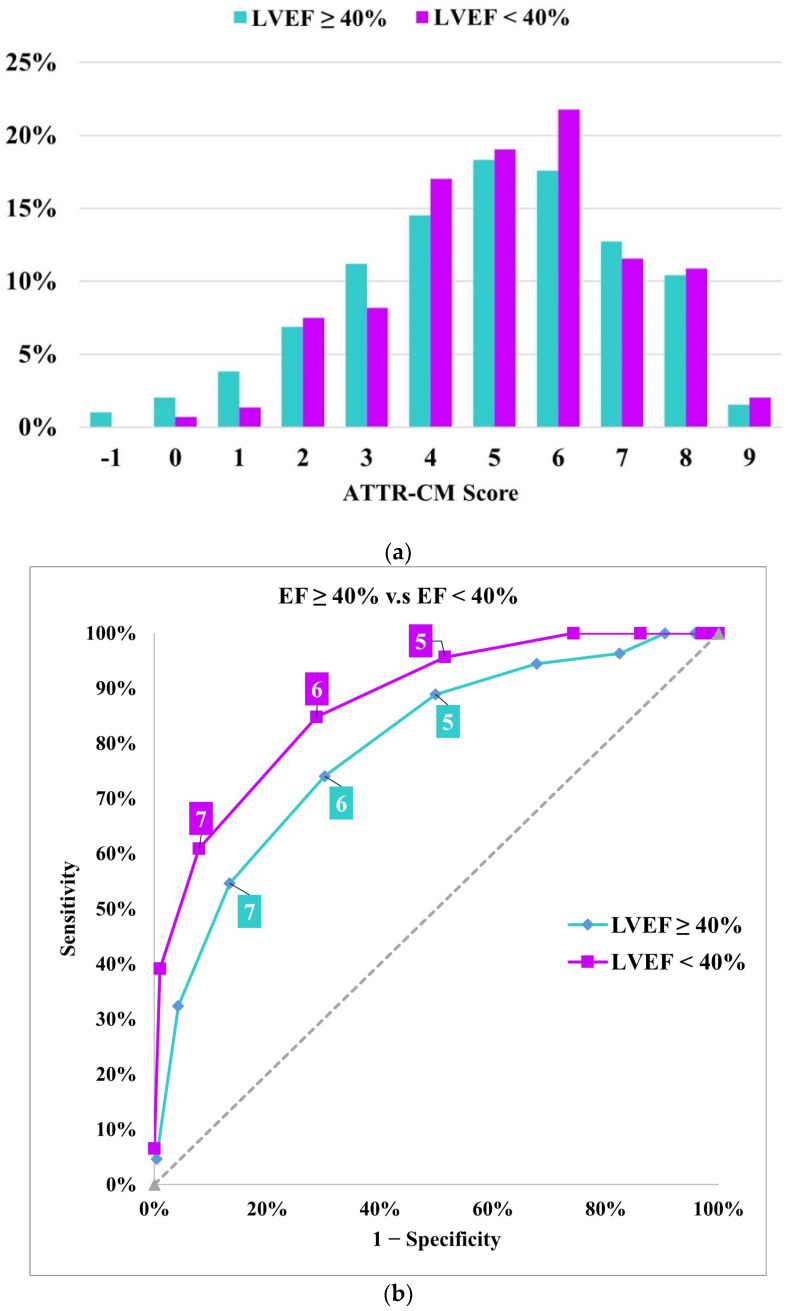
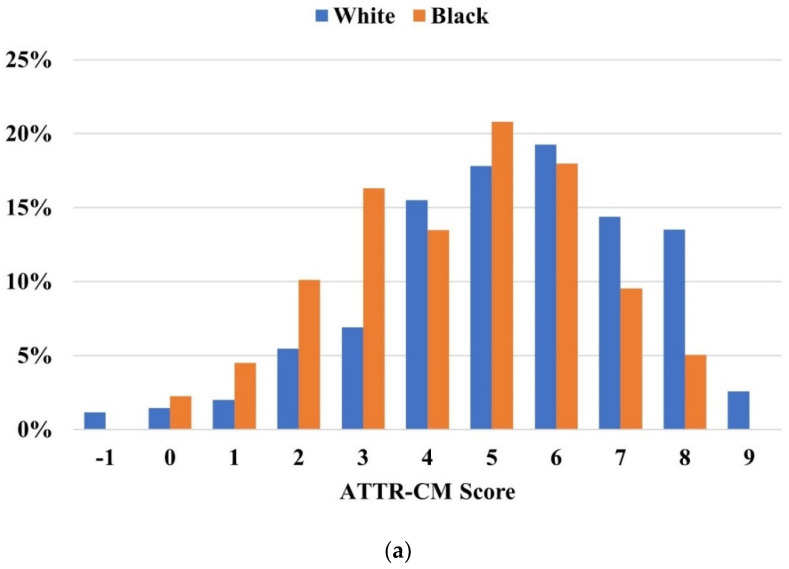
The early detection of transthyretin cardiac amyloidosis (ATTR-CM) is essential, with Tc-99m pyrophosphate scintigraphy (PYP scan) being a key diagnostic tool. Although a previously validated score has shown promise in predicting PYP scan positivity among patients with HFpEF, further evaluation in diverse cohorts is necessary. To assess the effectiveness of the ATTR-CM score in predicting PYP scan positivity within our patient population. We analyzed patients referred for PYP with SPECT at the Cleveland Clinic from January 2012 to January 2020, all of whom had undergone echocardiography within the previous year. The ATTR-CM score was determined using the following criteria: Age (60-69, +2; 70-79, +3; ≥80, +4), sex (male, +2), hypertension (present, -1), left ventricular ejection fraction (LVEF <60%, +1), posterior wall thickness (≥12 mm, +1), and relative wall thickness (>0.57, +2). A score of ≥6 indicated high risk. Among the 540 patients (32% female, 33% black), 27% had an LVEF <40%. The score demonstrated good discrimination by AUC, with consistent performance across different racial groups, sexes, and LVEF categories. For scores ≥6, sensitivity was lower in women and black patients; however, lowering the cutoff to 5 markedly improved sensitivity. The ATTR-CM score displayed consistently good performance by AUC across our cohort, including patients with HFrEF. Nevertheless, its sensitivity was reduced in black patients and women. Efforts to scale ATTR-CM diagnosis tools should be mindful of demographic differences in risk prediction models.
早期检测转甲状腺素蛋白心脏淀粉样变性(ATTR-CM)至关重要,锝-99m焦磷酸盐闪烁扫描(PYP扫描)是关键的诊断工具。尽管先前验证的评分在预测射血分数保留的心力衰竭(HFpEF)患者PYP扫描阳性方面显示出前景,但仍需要在不同队列中进行进一步评估。为了评估ATTR-CM评分在预测我们患者群体中PYP扫描阳性的有效性。我们分析了2012年1月至2020年1月在克利夫兰诊所因PYP单光子发射计算机断层扫描(SPECT)而转诊的患者,所有患者在前一年均接受了超声心动图检查。ATTR-CM评分根据以下标准确定:年龄(60 - 69岁,+2;70 - 79岁,+3;≥80岁,+4),性别(男性,+2),高血压(存在,-1),左心室射血分数(LVEF<60%,+1),后壁厚度(≥12mm,+1),以及相对壁厚度(>0.57,+2)。评分≥6表示高风险。在540例患者中(32%为女性,33%为黑人),27%的患者LVEF<40%。该评分通过曲线下面积(AUC)显示出良好的区分能力,在不同种族、性别和LVEF类别中表现一致。对于评分≥6的情况,女性和黑人患者的敏感性较低;然而,将临界值降低到5可显著提高敏感性。在我们的队列中,包括射血分数降低的心力衰竭(HFrEF)患者,ATTR-CM评分通过AUC始终显示出良好的性能。尽管如此,其在黑人患者和女性中的敏感性降低。扩大ATTR-CM诊断工具应用的努力应注意风险预测模型中的人口统计学差异。