Clinical Research Centre, (Hospital Queen Elizabeth II), Institute for Clinical Research, National Institute of Health, Ministry of Health Malaysia, Kota Kinabalu, Sabah, Malaysia.
Centre for Health Economics Research, Institute of Health Systems Research, National Institute of Health, Ministry of Health Malaysia, Kota Kinabalu, Sabah, Malaysia.
PLoS One. 2024 Oct 31;19(10):e0313131. doi: 10.1371/journal.pone.0313131. eCollection 2024.
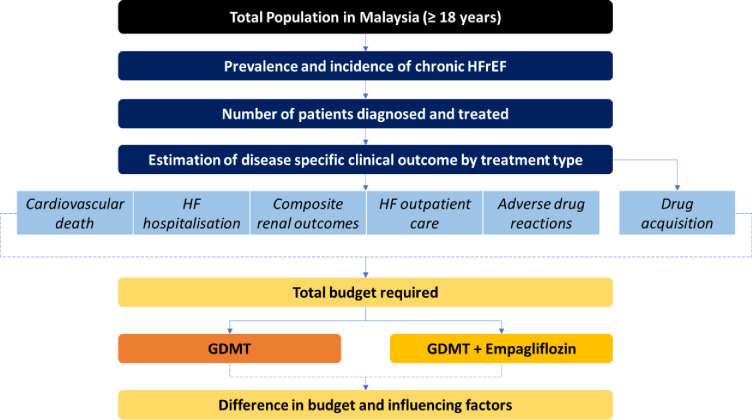
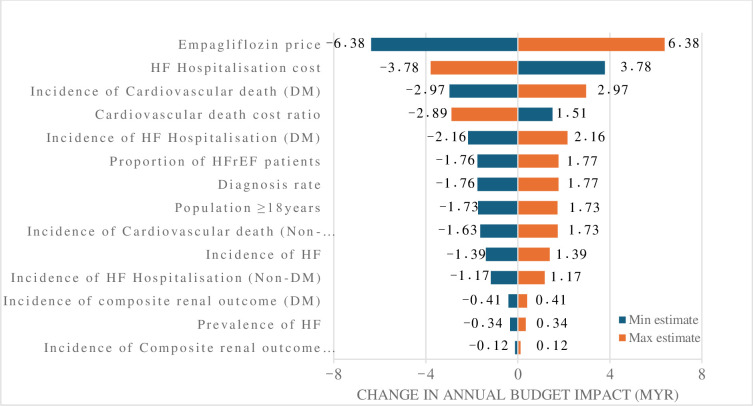
Sodium-glucose co-transporter-2 (SGLT2) inhibitors such as Empagliflozin, are increasingly recommended as part of guideline-directed medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF) in many developed nations. This recommendation is based on robust clinical evidence showing that adding Empagliflozin to GDMT improves heart failure symptoms, clinical outcomes, functional status, and overall quality of life. In Malaysia, where healthcare is predominantly public and heavily subsidized, the introduction of new treatments can significantly impact costs, requiring detailed economic assessments. This study evaluates the budget impact of incorporating Empagliflozin into GDMT for HFrEF from the perspective of the public healthcare system. A five-year budget impact model was developed, integrating local data such as population, drug use, costs, clinical outcomes, and healthcare expenses. In the current scenario (GDMT alone), the projected five-year expenditure is MYR 6.12 billion (USD 3.92 billion). With Empagliflozin, the total cost rises by 0.71% to MYR 6.16 billion (USD 3.95 billion), driven by drug acquisition costs of MYR 160.12 million (USD 102.64 million) and adverse event costs of MYR 211,543 (USD 135,604). However, these costs are offset by savings from reduced HF hospitalizations, fewer cardiovascular deaths, and improved renal outcomes. Sensitivity analysis identified hospitalization costs, the price of Empagliflozin, and cardiovascular deaths in diabetic patients as key factors influencing the budget impact. Policymakers can improve the affordability of Empagliflozin through strategies like price negotiations, cost-sharing, and focusing on high-risk groups to optimize healthcare expenditure while ensuring effective treatment access.
钠-葡萄糖协同转运蛋白 2(SGLT2)抑制剂,如恩格列净,在许多发达国家,作为射血分数降低的心力衰竭(HFrEF)指南指导的医学治疗(GDMT)的一部分,越来越被推荐。这一推荐是基于强有力的临床证据,表明在 GDMT 中加入恩格列净可改善心力衰竭症状、临床结局、功能状态和整体生活质量。在马来西亚,医疗保健主要是公共的,并得到大量补贴,新治疗方法的引入可能会对成本产生重大影响,需要进行详细的经济评估。本研究从公共医疗保健系统的角度评估了将恩格列净纳入 HFrEF 的 GDMT 的预算影响。开发了一个为期五年的预算影响模型,整合了当地数据,如人口、药物使用、成本、临床结局和医疗保健费用。在当前情况下(仅 GDMT),预计五年支出为 61.2 亿林吉特(39.2 亿美元)。随着恩格列净的加入,总费用增加了 0.71%,达到 61.6 亿林吉特(39.5 亿美元),这主要是由于药物采购成本增加了 1.6012 亿林吉特(1.0264 亿美元)和不良事件成本增加了 211543 林吉特(135604 美元)。然而,这些成本被因心力衰竭住院减少、心血管死亡减少和肾功能改善而节省的费用所抵消。敏感性分析确定住院费用、恩格列净的价格和糖尿病患者的心血管死亡是影响预算影响的关键因素。政策制定者可以通过价格谈判、成本分担和关注高风险群体等策略来提高恩格列净的可负担性,以优化医疗保健支出,同时确保有效的治疗机会。