Ong Siew Chin, Low Joo Zheng, Yew Wing Yee, Yen Chia How, Abdul Kader Muhamad Ali S K, Liew Houng Bang, Abdul Ghapar Abdul Kahar
Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, Pulau Pinag, Malaysia.
Hospital Sultan Ismail Petra, Ministry of Health, Kelantan, Malaysia.
Front Cardiovasc Med. 2022 Nov 2;9:971592. doi: 10.3389/fcvm.2022.971592. eCollection 2022.
Estimation of the economic burden of heart failure (HF) through a complete evaluation is essential for improved treatment planning in the future. This estimation also helps in reimbursement decisions for newer HF treatments. This study aims to estimate the cost of HF treatment in Malaysia from the Ministry of Health's perspective.
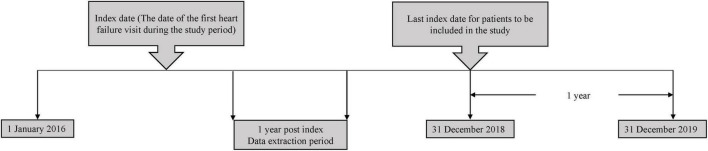
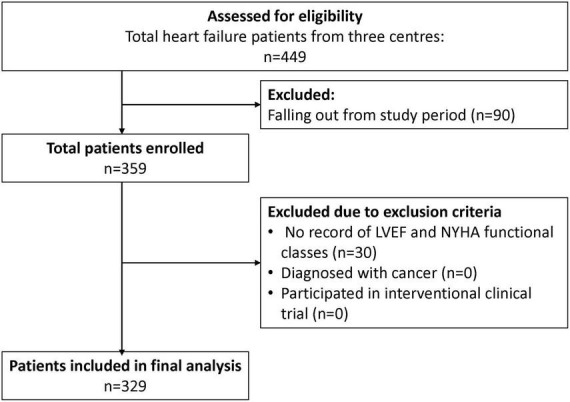
A prevalence-based, bottom-up cost analysis study was conducted in three tertiary hospitals in Malaysia. Chronic HF patients who received treatment between 1 January 2016 and 31 December 2018 were included in the study. The direct cost of HF was estimated from the patients' healthcare resource utilisation throughout a one-year follow-up period extracted from patients' medical records. The total costs consisted of outpatient, hospitalisation, medications, laboratory tests and procedure costs, categorised according to ejection fraction (EF) and the New York Heart Association (NYHA) functional classification.
A total of 329 patients were included in the study. The mean ± standard deviation of total cost per HF patient per-year (PPPY) was USD 1,971 ± USD 1,255, of which inpatient cost accounted for 74.7% of the total cost. Medication costs (42.0%) and procedure cost (40.8%) contributed to the largest proportion of outpatient and inpatient costs. HF patients with preserved EF had the highest mean total cost of PPPY, at USD 2,410 ± USD 1,226. The mean cost PPPY of NYHA class II was USD 2,044 ± USD 1,528, the highest among all the functional classes. Patients with underlying coronary artery disease had the highest mean total cost, at USD 2,438 ± USD 1,456, compared to other comorbidities. HF patients receiving angiotensin-receptor neprilysin-inhibitor (ARNi) had significantly higher total cost of HF PPPY in comparison to patients without ARNi consumption (USD 2,439 vs. USD 1,933, < 0.001). Hospitalisation, percutaneous coronary intervention, coronary angiogram, and comorbidities were the cost predictors of HF.
Inpatient cost was the main driver of healthcare cost for HF. Efficient strategies for preventing HF-related hospitalisation and improving HF management may potentially reduce the healthcare cost for HF treatment in Malaysia.
通过全面评估来估计心力衰竭(HF)的经济负担对于未来改进治疗规划至关重要。这种估计也有助于做出关于新型HF治疗的报销决策。本研究旨在从马来西亚卫生部的角度估计HF治疗的成本。
在马来西亚的三家三级医院开展了一项基于患病率的自下而上成本分析研究。纳入2016年1月1日至2018年12月31日期间接受治疗的慢性HF患者。HF的直接成本是根据从患者病历中提取的为期一年的随访期间患者的医疗资源利用情况来估计的。总成本包括门诊、住院、药物、实验室检查和手术费用,根据射血分数(EF)和纽约心脏协会(NYHA)功能分级进行分类。
本研究共纳入329例患者。每位HF患者每年的平均总成本(PPPY)为1971美元±1255美元,其中住院成本占总成本的74.7%。药物成本(42.0%)和手术成本(40.8%)在门诊和住院成本中占比最大。EF保留的HF患者的PPPY平均总成本最高,为2410美元±1226美元。NYHA II级的PPPY平均成本为2044美元±1528美元,在所有功能分级中最高。与其他合并症相比,患有潜在冠状动脉疾病的患者平均总成本最高,为2438美元±1456美元。与未使用血管紧张素受体脑啡肽酶抑制剂(ARNi)的患者相比,接受ARNi治疗的HF患者的HF PPPY总成本显著更高(2439美元对1933美元,<0.001)。住院、经皮冠状动脉介入治疗、冠状动脉造影和合并症是HF的成本预测因素。
住院成本是HF医疗成本的主要驱动因素。预防HF相关住院和改善HF管理的有效策略可能会降低马来西亚HF治疗的医疗成本。