Department of Endocrinology, Beijing Tongren Hospital CMU, Beijing, China.
Maastricht University Medical Centre, Maastricht, Netherlands.
BMJ Open. 2024 Nov 1;14(10):e075955. doi: 10.1136/bmjopen-2023-075955.
This study aimed to examine the relationship between measures of kidney function and impaired lung function in individuals with diabetes and to assess all-cause mortality risk associated with having chronic kidney disease (CKD) and or impaired lung function.
Cross-sectional and retrospective cohort study.
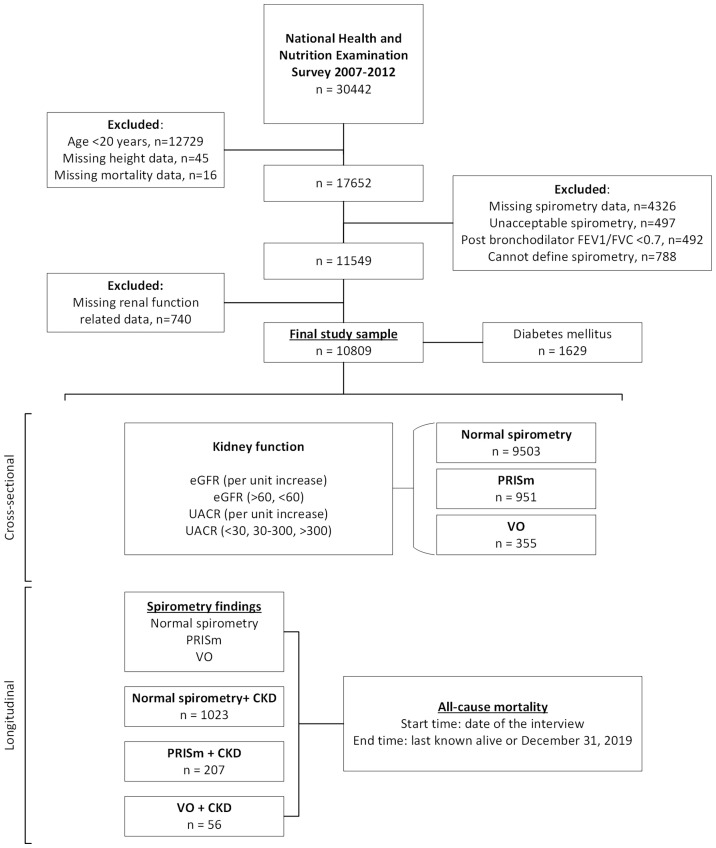
The National Health and Nutrition Examination Survey 2007-2012.
A total of 10 809 participants aged over 20 years were included in this study: 9503 with normal spirometry, 951 with preserved ratio impaired spirometry (PRISm) and 355 with variable obstruction (VO).
Kidney function measures, including estimated glomerular filtration rate (eGFR) and urinary albumin to creatinine ratio (UACR), were considered exposure variables. PRISm and VO were outcome variables. PRISm was defined as a forced expiratory volume in 1 s (FEV1)<80% predicted and an FEV1/forced vital capacity (FVC) ratio≥0.7, while VO was defined as an FEV1/FVC ratio <0.7 prebronchodilator and ≥0.7 postbronchodilator. In the cross-sectional analysis, multivariate logistic regression models were used to assess the relationship between kidney function measures and spirometry findings. In the retrospective cohort analysis, Cox proportional hazards models were employed to evaluate the impact of having PRISm or VO, combined with CKD, on all-cause mortality.
An increase in UACR was significantly associated with higher odds of PRISm (OR (95% CI)=1.10 (1.01, 1.21), p=0.03). Additionally, eGFR <60 was associated with the odds of variable obstructive lung function (OR (95% CI)=1.72 (1.07, 2.74), p=0.03) compared with eGFR >60. After adjustments, an increase in UACR was associated with higher odds of PRISm in individuals with diabetes (OR (95% CI)=1.21 (1.08, 1.36), p=0.002), and UACR ≥300 mg/g significantly increased odds of having PRISm in idividuals with diabetes (OR (95% CI)=2.34 (1.23, 4.47), p=0.01). During a mean follow-up of 12.3 years, 10 500 deaths occurred. In the diabetic group, compared with normal spirometry without CKD, those with both PRISm and CKD had a significantly increased risk of all-cause mortality (HR (95% CI)=3.46 (1.94, 6.16), p<0.0001).
An elevated UACR and albuminuria were linked to a higher risk of PRISm. Our study emphasises that kidney and lung function are correlated. Further research is necessary to confirm our findings.
本研究旨在探讨糖尿病患者肾功能指标与肺功能受损之间的关系,并评估合并慢性肾脏病(CKD)和/或肺功能受损与全因死亡率的相关性。
横断面和回顾性队列研究。
2007-2012 年全国健康和营养调查。
本研究共纳入 10809 名年龄超过 20 岁的参与者:9503 名肺功能正常,951 名比预计比值受损的肺功能(PRISm)和 355 名可变阻塞(VO)。
包括估计肾小球滤过率(eGFR)和尿白蛋白/肌酐比值(UACR)在内的肾功能指标被视为暴露变量。PRISm 和 VO 是结局变量。PRISm 定义为 1 秒用力呼气量(FEV1)<80%预计值和 FEV1/用力肺活量(FVC)比值≥0.7,而 VO 定义为支气管扩张剂前 FEV1/FVC 比值<0.7 且≥0.7。在横断面分析中,使用多变量逻辑回归模型评估肾功能指标与肺功能检查结果之间的关系。在回顾性队列分析中,采用 Cox 比例风险模型评估 PRISm 或 VO 合并 CKD 对全因死亡率的影响。
UACR 升高与 PRISm 的比值比(OR)显著相关(95% CI=1.10(1.01,1.21),p=0.03)。此外,与 eGFR>60 相比,eGFR<60 与可变阻塞性肺功能的比值比(OR(95% CI)=1.72(1.07,2.74),p=0.03)相关。调整后,UACR 升高与糖尿病患者 PRISm 的比值比(OR(95% CI)=1.21(1.08,1.36),p=0.002)相关,UACR≥300mg/g 显著增加了糖尿病患者 PRISm 的比值比(OR(95% CI)=2.34(1.23,4.47),p=0.01)。在平均 12.3 年的随访期间,有 10500 人死亡。在糖尿病组中,与无 CKD 的正常肺功能相比,同时患有 PRISm 和 CKD 的患者全因死亡率的风险显著增加(HR(95% CI)=3.46(1.94,6.16),p<0.0001)。
UACR 和白蛋白尿的升高与 PRISm 的风险增加相关。我们的研究强调了肾脏和肺部功能是相关的。需要进一步的研究来证实我们的发现。