Sarah Cannon Research Institute, 250 25th Avenue North, Nashville, TN, 37203, USA.
Sarah Cannon Research Institute at HealthONE, Denver, CO, USA.
Target Oncol. 2024 Nov;19(6):879-892. doi: 10.1007/s11523-024-01102-8. Epub 2024 Nov 1.
Adavosertib is a first-in-class, selective small-molecule inhibitor of Wee1. Olaparib is an inhibitor of poly(ADP-ribose) polymerase (PARP). Preclinical data suggest that adavosertib enhances the antitumor effect of PARP inhibitors.
The safety, tolerability, and efficacy of adavosertib plus olaparib were evaluated in patients with refractory solid tumors to define the maximum tolerated dose (MTD) and recommended phase II dose (RP2D).
Eligible patients in part A (dose finding) had a refractory solid tumor for which there is no established treatment and had received ≥ 1 prior course of systemic therapy; in part B (dose expansion), patients had platinum-sensitive extensive-stage or relapsed small-cell lung cancer (SCLC). Patients received adavosertib [once (qd) or twice daily (bid)] for 3 consecutive days with 4 days off treatment (3/4), or 5 consecutive days with 2 days off (5/2), plus olaparib (bid) for 14 or 21 days of a 21-day cycle.
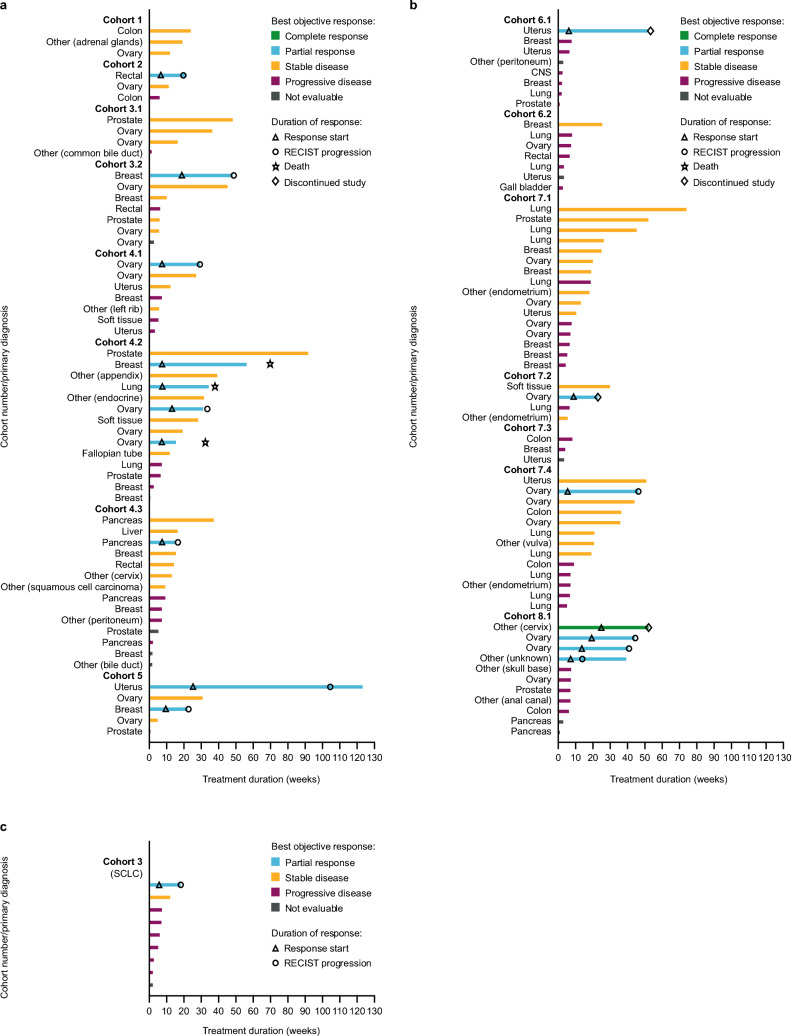
A total of 130 patients were enrolled in the study, 120 in part A and 10 in part B. The MTD for adavosertib bid was 175 mg (days 1-3, 8-10/21-day cycle) plus continuous olaparib 200 mg bid; the once-daily MTD (and RP2D) was adavosertib 200 mg (days 1-3, 8-10/21-day cycle) plus continuous olaparib 200 mg bid. In the MTD/RP2D cohort, one patient (7%) experienced a dose-limiting toxicity (DLT) of thrombocytopenia. The most common treatment-related adverse events (TRAEs) in the cohorts in which MTD/RP2D for bid dosing and RP2D for qd dosing were determined were fatigue (64.3% and 15.4%, respectively), diarrhea (42.9% and 30.8%), decreased appetite (35.7% and 23.1%), nausea (35.7% and 15.4%), and anemia (35.7% and 38.5%). In the SCLC dose-expansion cohort, TRAEs occurred in eight patients (88.9%), including thrombocytopenia (66.7%) and anemia (55.6%). In part A, objective response rate (ORR) was 14.8% [95% confidence interval (CI) 8.7-22.9] overall; for the cohorts in which MTD/RP2D for bid dosing and RP2D for qd dosing were determined, ORR was 30.8% (9.1-61.4) and 9.1% (0.2-41.3), respectively. ORR was 11.1% [95% CI 0.3-48.2; one partial response (PR)], disease control rate was 22.2% (2.8-60.0; one PR, one stable disease), and median progression-free survival was 1.5 months (1.3-4.2) in the SCLC dose-expansion cohort.
Adverse events and DLTs observed in the bid MTD and once-daily MTD/RP2D dosing schedules were manageable and consistent with known adavosertib and olaparib safety profiles. Limited antitumor activity was observed with adavosertib plus olaparib combination therapy.
ClinicalTrials.gov, NCT02511795 (registration: 28 July 2015).
Adavosertib 是一种首创的、选择性的 Wee1 小分子抑制剂。奥拉帕利是一种聚(ADP-核糖)聚合酶(PARP)抑制剂。临床前数据表明,adavosertib 增强了 PARP 抑制剂的抗肿瘤作用。
评估 adavosertib 联合奥拉帕利在难治性实体瘤患者中的安全性、耐受性和疗效,以确定最大耐受剂量(MTD)和推荐的 II 期剂量(RP2D)。
A 部分(剂量发现)的合格患者患有难治性实体瘤,没有既定的治疗方法,并且已经接受了≥1 次系统治疗;B 部分(剂量扩展)的患者患有铂敏感广泛期或复发性小细胞肺癌(SCLC)。患者接受 adavosertib [qd 或 bid,连续 3 天,停药 4 天(3/4),或连续 5 天,停药 2 天(5/2)],加上奥拉帕利(bid),21 天周期中 14 或 21 天。
共有 130 名患者入组研究,120 名在 A 部分,10 名在 B 部分。adavosertib bid 的 MTD 为 175mg(第 1-3 天,第 8-10/21 天周期),加连续奥拉帕利 200mg bid;qd 的单次 MTD(和 RP2D)为 adavosertib 200mg(第 1-3 天,第 8-10/21 天周期),加连续奥拉帕利 200mg bid。在 MTD/RP2D 队列中,1 名患者(7%)出现血小板减少症的剂量限制毒性(DLT)。在确定 bid 剂量的 MTD/RP2D 和 qd 剂量的 RP2D 的队列中,最常见的治疗相关不良事件(TRAEs)是疲劳(64.3%和 15.4%)、腹泻(42.9%和 30.8%)、食欲下降(35.7%和 23.1%)、恶心(35.7%和 15.4%)和贫血(35.7%和 38.5%)。在 SCLC 剂量扩展队列中,8 名患者(88.9%)出现 TRAEs,包括血小板减少症(66.7%)和贫血(55.6%)。在 A 部分,总体客观缓解率(ORR)为 14.8%[95%置信区间(CI)8.7-22.9];在确定 bid 剂量的 MTD/RP2D 和 qd 剂量的 RP2D 的队列中,ORR 分别为 30.8%(9.1-61.4)和 9.1%(0.2-41.3)。在 SCLC 剂量扩展队列中,ORR 为 11.1%[95%CI 0.3-48.2;1 例部分缓解(PR)],疾病控制率为 22.2%(2.8-60.0;1 例 PR,1 例稳定疾病),中位无进展生存期为 1.5 个月(1.3-4.2)。
在 bid MTD 和 qd MTD/RP2D 剂量方案中观察到的不良事件和 DLT 是可以控制的,与已知的 adavosertib 和奥拉帕利安全性特征一致。adavosertib 联合奥拉帕利联合治疗观察到有限的抗肿瘤活性。
ClinicalTrials.gov,NCT02511795(注册日期:2015 年 7 月 28 日)。