Denham Nathan C, Selvaraj Raja, Kakarla Jayant, Patloori Sirish Chandra Srinath, Roche S Lucy, Thorne Sara, Oechslin Erwin, Massarella Danielle, Wald Rachel, Alonso-Gonzalez Rafael, Silversides Candice, Downar Eugene, Nair Krishnakumar
University Health Network Toronto, Peter Munk Cardiac Centre, and University of Toronto, Toronto, Ontario, Canada.
Department of Cardiology, JIPMER, Puducherry, India.
JACC Adv. 2024 Oct 17;3(11):101329. doi: 10.1016/j.jacadv.2024.101329. eCollection 2024 Nov.
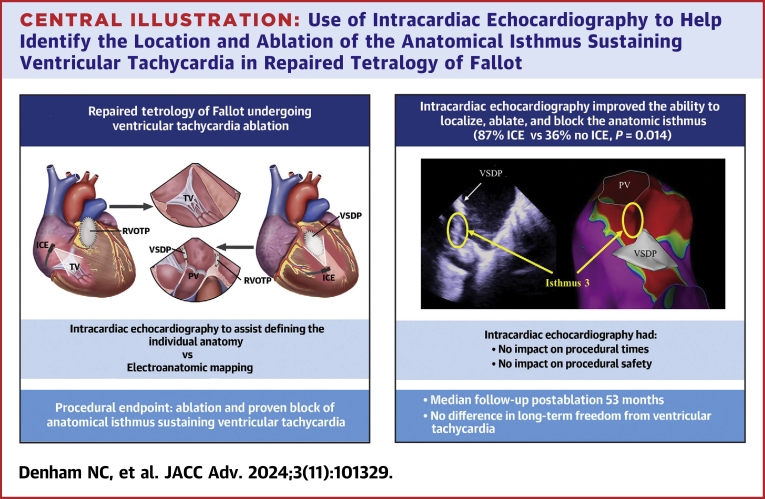
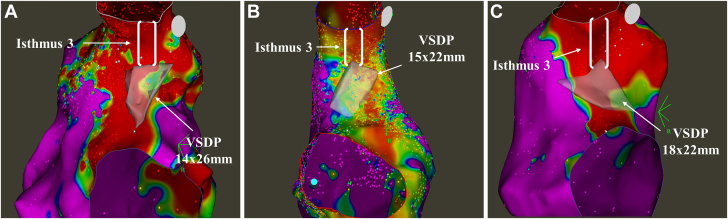
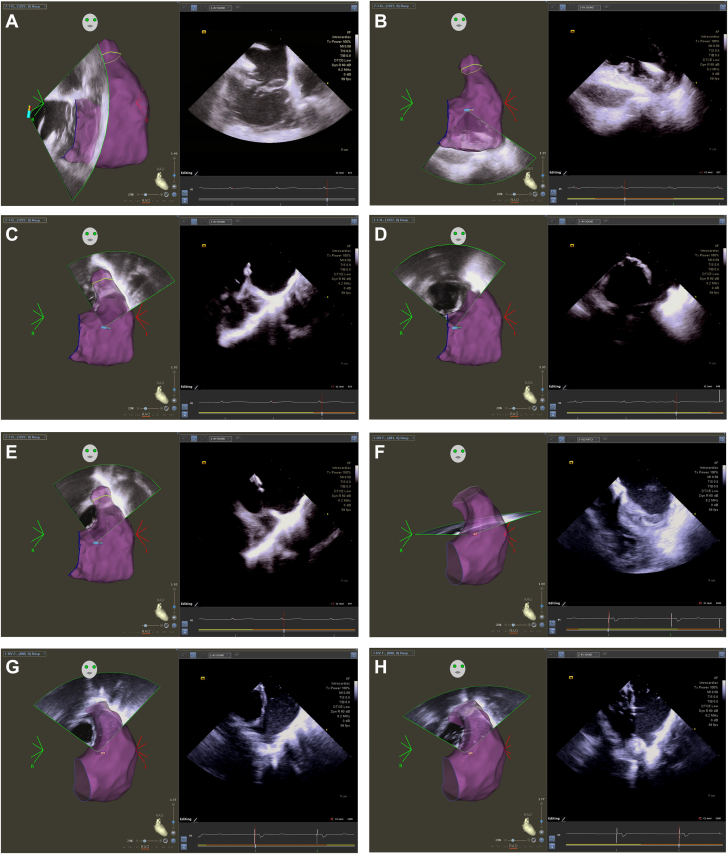
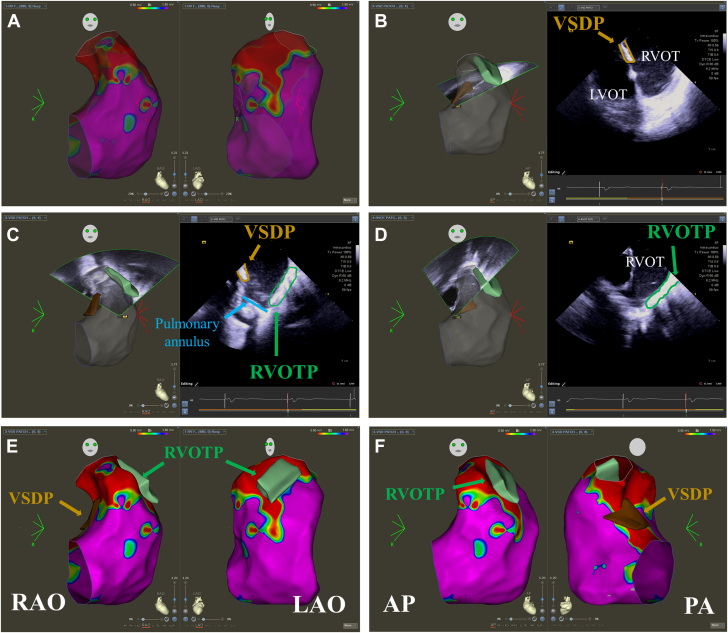
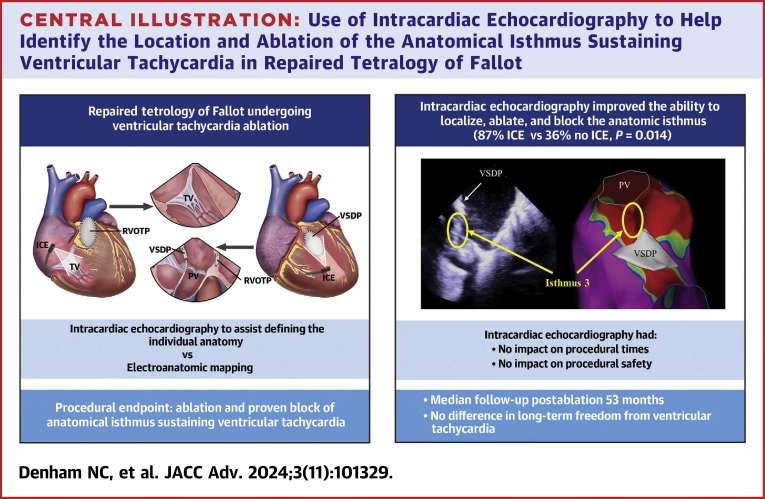
Successful catheter ablation of ventricular tachycardia (VT) in repaired tetralogy of Fallot (TOF) can be achieved by targeting 1 or more anatomical isthmuses. However, significant interindividual variability in the size and location of surgical patches means careful mapping is required to design ablation lines to block the isthmus. Intracardiac echocardiography (ICE) may assist ablation by accurate identification of individual TOF anatomy.
The authors hypothesized ICE-guided VT ablation improved isthmus recognition, ablation, and procedural outcomes.
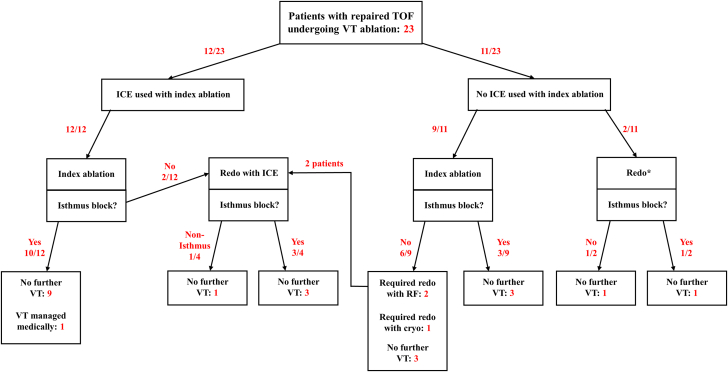
Retrospective study of adults with repaired TOF undergoing VT ablation between January 1, 2017 and December 31, 2022. ICE integration was compared to a strategy using electroanatomical mapping only to identify anatomic boundaries. All cases underwent ablation and had proven isthmus block as the procedural endpoint.
Twenty-three patients (age 47 ± 14 years; 61% male) underwent 27 VT ablations (ICE: 16/27 [59%]; no ICE: 11/27 [41%]). ICE improved the ability to localize and ablate the anatomical isthmus (ICE: 13/15 [87%] vs no ICE: 4/11 [36%]; = 0.014); however, there was no difference in long-term freedom from VT (ICE: 9/12 [75%] vs no ICE: 8/11 [73%]; = 0.901). ICE had no impact on procedural times (ICE: 173 ± 48 minutes vs no ICE: 157 ± 47 minutes; = 0.399), fluoroscopy time (ICE: 30 ± 16 minutes vs no ICE: 29 ± 10 minutes; = 0.864), or major complications (ICE: 1/16 [6%] vs no ICE 0/11; = 1.000).
ICE improves ablation of the anatomical isthmus for sustaining VT in patients with repaired TOF by demonstrating the individual anatomy but does not improve long-term outcomes.
通过靶向1个或更多解剖峡部,可成功对法洛四联症(TOF)修复术后的室性心动过速(VT)进行导管消融。然而,手术补片的大小和位置存在显著个体差异,这意味着需要仔细标测以设计消融线来阻断峡部。心腔内超声心动图(ICE)可通过准确识别个体TOF解剖结构来辅助消融。
作者假设ICE引导的VT消融可改善峡部识别、消融及手术结果。
对2017年1月1日至2022年12月31日期间接受VT消融的TOF修复术后成年患者进行回顾性研究。将ICE整合与仅使用电解剖标测来识别解剖边界的策略进行比较。所有病例均接受消融,并以证实峡部阻滞作为手术终点。
23例患者(年龄47±14岁;61%为男性)接受了27次VT消融(ICE组:16/27 [59%];非ICE组:11/27 [41%])。ICE提高了定位和消融解剖峡部的能力(ICE组:13/15 [87%] 对比非ICE组:4/11 [36%];P = 0.014);然而,VT长期缓解率无差异(ICE组:9/12 [75%] 对比非ICE组:8/11 [73%];P = 0.901)。ICE对手术时间(ICE组:173±48分钟对比非ICE组:157±47分钟;P = 0.399)、透视时间(ICE组:30±16分钟对比非ICE组:29±10分钟;P = 0.864)或主要并发症(ICE组:1/16 [6%] 对比非ICE组0/11;P = 1.000)均无影响。
ICE通过显示个体解剖结构,改善了TOF修复术后患者持续性VT的解剖峡部消融,但未改善长期结果。