Abgrall S, Selinger-Leneman H, Lanoy E, Becker A, Matheron S, de Truchis P, Pavie J, Canestri A, Khuong M A, Rey D, Caby F, Tattevin P, Palich R, Grabar S
AP-HP, Hôpital Béclère, Service de Médecine Interne, Clamart, and Université Paris-Saclay, CESP INSERM U1018, Le Kremlin-Bicêtre, France.
Sorbonne Université, INSERM, Institut Pierre Louis d'Epidémiologie et de Santé Publique, Paris, France.
HIV Med. 2025 Feb;26(2):252-264. doi: 10.1111/hiv.13729. Epub 2024 Nov 4.
Assessing the potential increased risk of viral rebound (VR) in migrants requires adequate control for sex and acquisition risk groups.
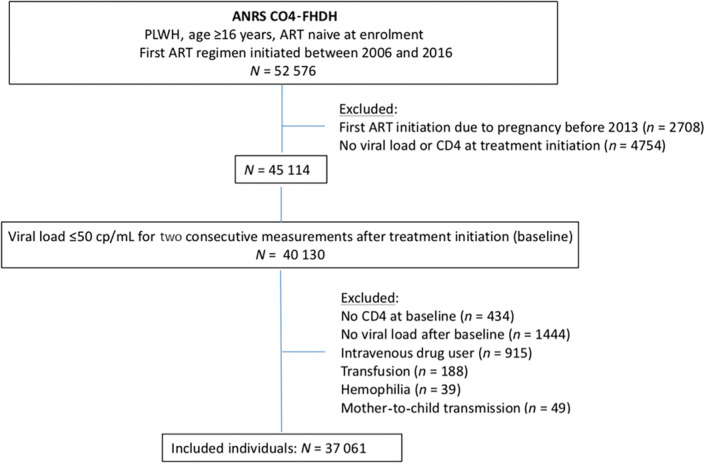
People living with HIV1, enrolled in the ANRS CO4-French Hospital Database on HIV, who achieved virological suppression with antiretroviral therapy (ART) initiated between 2006 and 2016 were included. We first compared the risk of VR, with loss to follow-up and death considered as competing events, across origin among the HIV acquisition groups, then across acquisition groups among the different origins, and finally across modality of a variable combining sex, acquisition group, and origin. Models were adjusted for clinical and biological confounding factors.
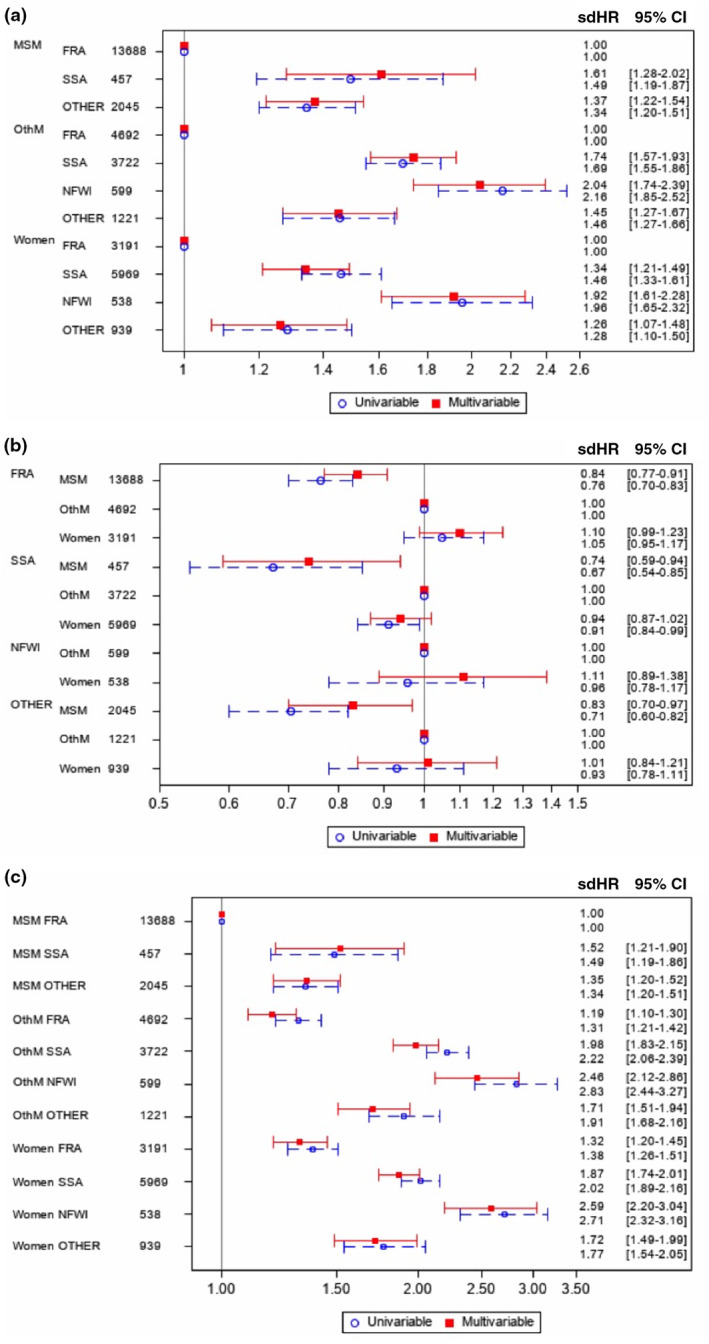
We included 21 571 French natives (FRA), 10 148 migrants from sub-Saharan Africa (SSA), 1137 migrants from the non-French West Indies (NFWI), and 4205 other migrants (OTHER). The 5-year probability of VR was 19% (95% confidence interval [CI] 19-20) overall, 15% in FRA, 21% in OTHER, 26% in SSA, and 34% in NFWI (p < 0.0001). It was 14% in men who have sex with men (MSM), 23% in heterosexual men, and 23% in women (p < 0.0001). After adjustment, all acquisition groups had a higher risk of VR than MSM from FRA, with men and women from NFWI having the highest risk (adjusted hazard ratio [aHR] 2.46; 95% CI 2.12-2.86 and aHR 2.59; 95% CI 2.20-3.04, respectively). Within each acquisition group, all groups of origin had a higher risk of VR than FRA. Within each region of origin, except the NFWI, heterosexual men had a higher risk of VR than MSM.
After accounting for sex and acquisition group, migration, especially from NFWI, remains prognostic of VR.
评估移民中病毒反弹(VR)潜在增加的风险需要对性别和感染风险群体进行充分控制。
纳入了参加ANRS CO4 - 法国医院HIV数据库的HIV - 1感染者,这些感染者在2006年至2016年期间开始接受抗逆转录病毒治疗(ART)并实现了病毒学抑制。我们首先比较了HIV感染群体中不同来源的VR风险,并将失访和死亡视为竞争事件,然后比较了不同来源中不同感染群体的VR风险,最后比较了一个结合性别、感染群体和来源的变量的不同模式的VR风险。模型针对临床和生物学混杂因素进行了调整。
我们纳入了21571名法国本土人(FRA)、10148名撒哈拉以南非洲移民(SSA)、1137名非法属西印度群岛移民(NFWI)和4205名其他移民(OTHER)。总体而言,VR的5年概率为19%(95%置信区间[CI] 19 - 20),FRA为15%,OTHER为21%,SSA为26%,NFWI为34%(p < 0.0001)。男男性行为者(MSM)为14%,异性恋男性为23%,女性为23%(p < 0.0001)。调整后,所有感染群体的VR风险均高于FRA的MSM,NFWI的男性和女性风险最高(调整后风险比[aHR]分别为2.46;95% CI 2.12 - 2.86和aHR 2.59;95% CI 2.20 - 3.04)。在每个感染群体中,所有来源组的VR风险均高于FRA。在每个原籍地区域内,除NFWI外,异性恋男性的VR风险高于MSM。
在考虑性别和感染群体后,移民,尤其是来自NFWI的移民,仍然是VR的预后因素。