Lamoine Sylvain, Jury Vincent, Fourneyron Virginie, Douxfils Jonathan, Teissandier Dorian, Talon Laurie, Sinegre Thomas, Lebreton Aurélien
Hematology Department, University Hospital of Clermont-Ferrand, Clermont-Ferrand, France.
Department of Pharmacy, Clinical Pharmacology and Toxicology Research Unit, Namur Research Institute for Life Sciences (NARILIS), University of Namur, Namur, Belgium.
Res Pract Thromb Haemost. 2024 Sep 23;8(7):102576. doi: 10.1016/j.rpth.2024.102576. eCollection 2024 Oct.
The incidence of cardiovascular diseases is increasing in persons with hemophilia A (HA). Therefore, anticoagulant therapy based on direct oral anticoagulants (DOACs) may be needed, despite the bleeding risk. In case of surgery or bleeding, such patients may be concomitantly treated with emicizumab (routine prophylaxis), factor (F)VIII products, and DOAC. Their concomitant presence constitutes a hemostatic challenge. Recent international guidelines stated that data are scarce on the hemostatic balance of plasma samples from patients with HA receiving emicizumab and DOAC.
The aim of this observational study was to assess the coagulation of FVIII-deficient plasma spiked with DOAC and emicizumab and to evaluate the effects of FVIII addition.
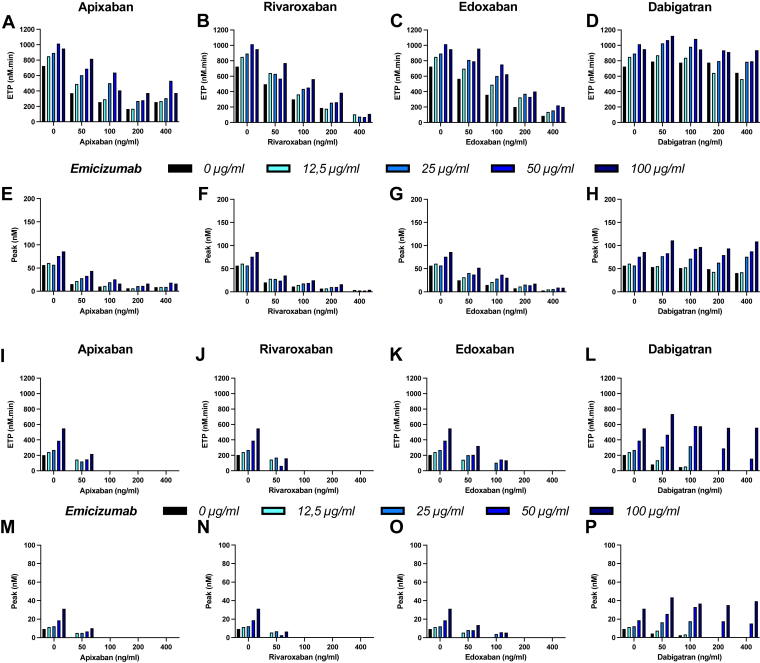
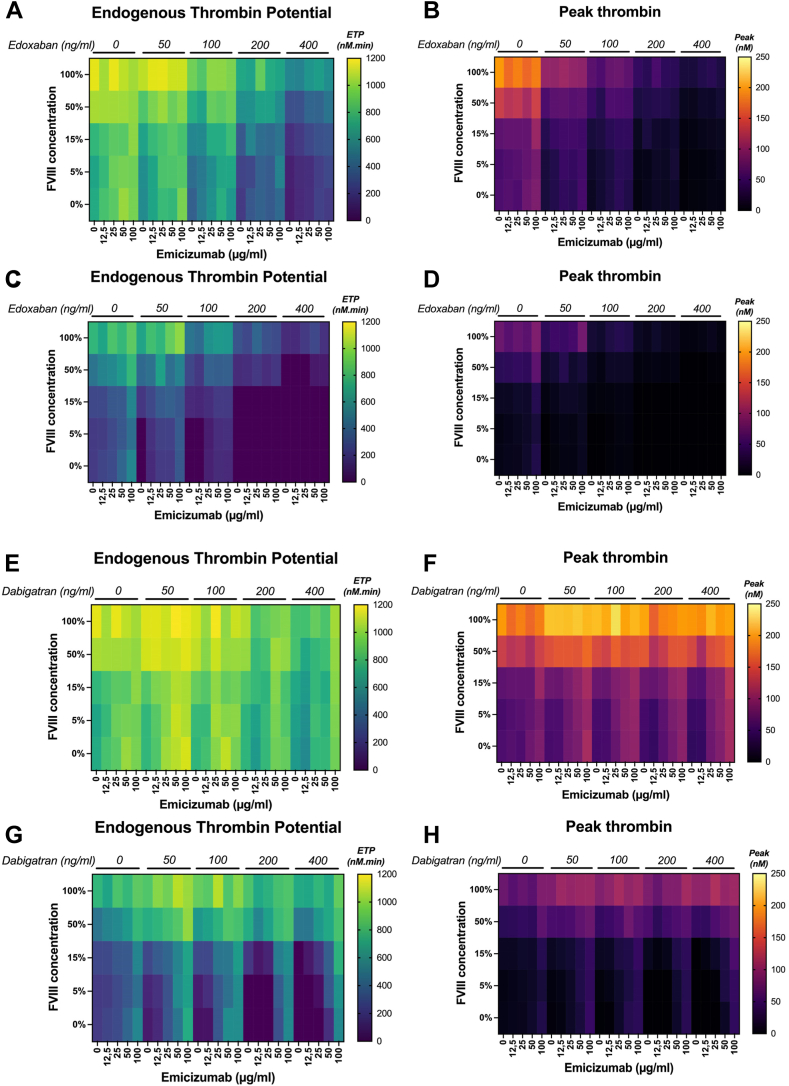
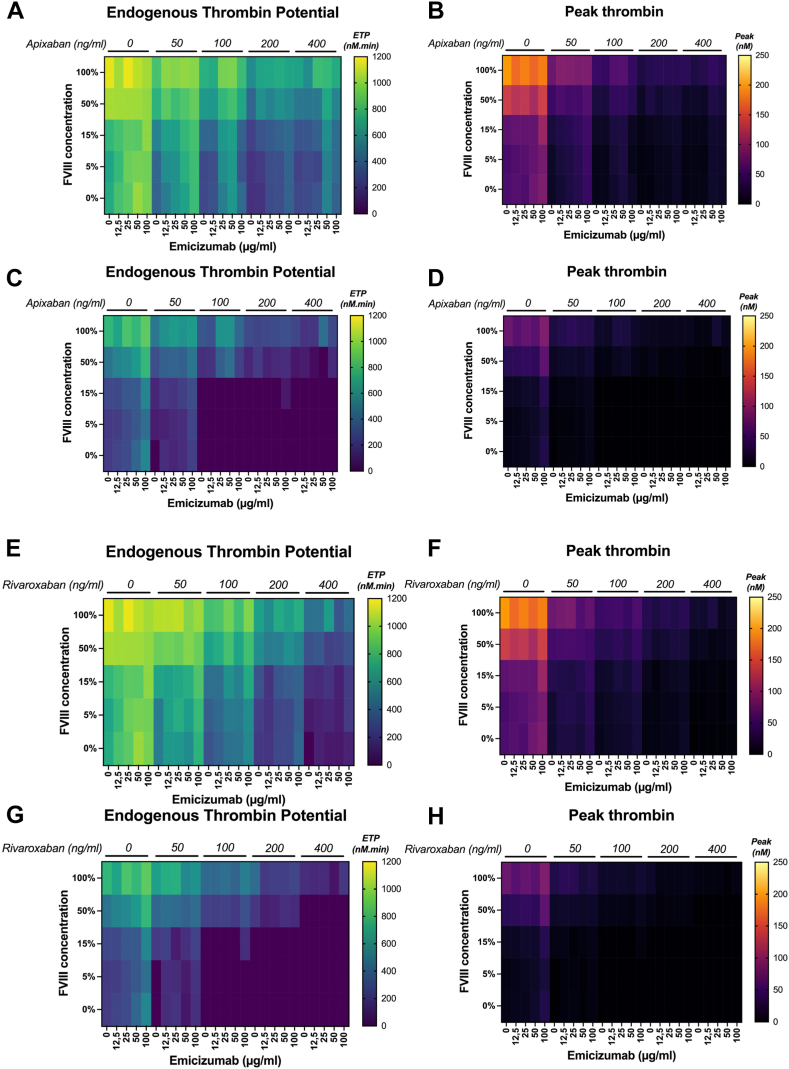
Prothrombin time, activated partial thromboplastin time, and thrombin generation (TG) using the calibrated automated thrombogram method were evaluated in aliquots of a commercial severe HA plasma supplemented with emicizumab (0, 12.5, 25, 50, and 100 ng/mL), DOAC (0, 50, 100, 200, and 400 ng/mL of apixaban, rivaroxaban, edoxaban, or dabigatran) and FVIII (0%, 5%, 15%, 50%, and 100%).
DOAC rapidly induced a TG decrease. Emicizumab could counter this effect only for the lowest DOAC dose. FVIII addition to the FVIII-deficient plasma containing a DOAC and emicizumab improved TG and countered the anticoagulant effect of DOAC at ≤100 ng/mL.
Our findings indicate that FVIII can be safely used with emicizumab to counter the anticoagulant effect of DOAC at ≤100 ng/mL. The TG assay is an efficient tool to monitor plasma containing anti-FXa DOAC, but not dabigatran (anti-FIIa).
甲型血友病(HA)患者心血管疾病的发病率正在上升。因此,尽管存在出血风险,可能仍需要基于直接口服抗凝剂(DOACs)的抗凝治疗。在手术或出血的情况下,此类患者可能同时接受艾美赛珠单抗(常规预防)、凝血因子(F)VIII产品和DOAC治疗。它们同时存在构成了止血挑战。最近的国际指南指出,关于接受艾美赛珠单抗和DOAC的HA患者血浆样本止血平衡的数据很少。
本观察性研究的目的是评估添加DOAC和艾美赛珠单抗的FVIII缺乏血浆的凝血情况,并评估添加FVIII的效果。
使用校准自动血栓图法,对添加了艾美赛珠单抗(0、12.5、25、50和100 ng/mL)、DOAC(阿哌沙班、利伐沙班、依度沙班或达比加群的0、50、100、200和400 ng/mL)和FVIII(0%、5%、15%、50%和100%)的市售重度HA血浆等分试样进行凝血酶原时间、活化部分凝血活酶时间和凝血酶生成(TG)评估。
DOAC迅速导致TG降低。艾美赛珠单抗仅能抵消最低DOAC剂量的这种作用。向含有DOAC和艾美赛珠单抗的FVIII缺乏血浆中添加FVIII可改善TG,并抵消≤100 ng/mL的DOAC的抗凝作用。
我们的研究结果表明,FVIII可与艾美赛珠单抗安全联用,以抵消≤100 ng/mL的DOAC的抗凝作用。TG检测是监测含抗FXa DOAC血浆的有效工具,但不适用于达比加群(抗FIIa)。