Byeon Jinyoung, Kang Eunhye, Jung Ji-Jung, Cheun Jong-Ho, Seo Kwan Sik, Kim Hong-Kyu, Lee Han-Byoel, Han Wonshik, Moon Hyeong-Gon
Department of Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
J Breast Cancer. 2024 Oct;27(5):323-333. doi: 10.4048/jbc.2024.0180.
Although numerous studies have identified potential risk factors for ipsilateral lymphedema development in patients with breast cancer following axillary node dissection, the risk factors for lymphedema in patients undergoing sentinel node biopsy without axillary dissection remain unclear. In this study, we aimed to determine the real-world incidence and risk factors for lymphedema in such patients.
We conducted a single-center, retrospective review of medical records of patients with breast cancer who underwent sentinel node biopsy alone. The development cohort (5,051 patients, January 2017-December 2020) was analyzed to identify predictors of lymphedema, and a predictive model was subsequently created. A validation cohort (1,627 patients, January 2014-December 2016) was used to validate the model.
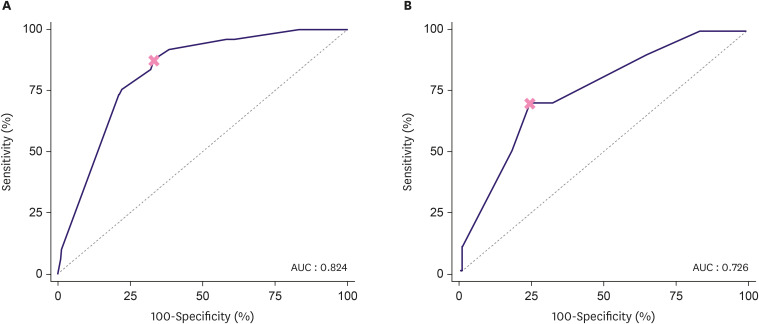
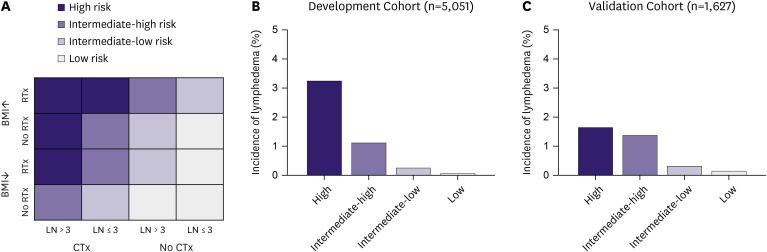
In the development cohort, 49 patients (0.9%) developed lymphedema over a median follow-up of 56 months, with most cases occurring within the first three years post-operation. Multivariate analysis revealed that a body mass index (BMI) of 30 kg/m² or above, radiation therapy (RTx), chemotherapy, and more than three harvested lymph nodes significantly predicted lymphedema. The predictive model showed an area under the curve of 0.824 for systemic chemotherapy, with the number of harvested lymph nodes being the most significant factor. Patients were stratified into four risk groups, showing lymphedema incidences of 3.3% in the highest-risk group and 0.1% in the lowest-risk group. In the validation cohort, the incidences were 1.7% and 0.2% for the highest and lowest risk groups, respectively.
The lymphedema prediction model identifies RTx, chemotherapy, BMI ≥ 30 kg/m², and more than three harvested lymph nodes as significant risk factors. Although the overall incidence is low, the risk is notably influenced by the extent of lymph node removal and systemic therapies. The model's high negative predictive value supports its application in designing tailored lymphedema surveillance programs for early intervention.
尽管众多研究已确定乳腺癌患者腋窝淋巴结清扫术后同侧淋巴水肿发生的潜在风险因素,但对于仅接受前哨淋巴结活检而未进行腋窝清扫的患者,淋巴水肿的风险因素仍不明确。在本研究中,我们旨在确定此类患者淋巴水肿的实际发生率及风险因素。
我们对仅接受前哨淋巴结活检的乳腺癌患者的病历进行了单中心回顾性研究。分析发展队列(2017年1月至2020年12月的5051例患者)以确定淋巴水肿的预测因素,随后创建了一个预测模型。使用验证队列(2014年1月至2016年12月的1627例患者)对该模型进行验证。
在发展队列中,49例患者(0.9%)在中位随访56个月时发生了淋巴水肿,大多数病例发生在术后的前三年。多因素分析显示,体重指数(BMI)≥30kg/m²、放疗(RTx)、化疗以及切除的淋巴结超过三个是淋巴水肿的显著预测因素。该预测模型对全身化疗的曲线下面积为0.824,其中切除的淋巴结数量是最显著的因素。患者被分为四个风险组,最高风险组的淋巴水肿发生率为3.3%,最低风险组为0.1%。在验证队列中,最高和最低风险组的发生率分别为1.7%和0.2%。
淋巴水肿预测模型确定放疗、化疗、BMI≥30kg/m²以及切除的淋巴结超过三个为显著风险因素。尽管总体发生率较低,但风险受淋巴结切除范围和全身治疗的显著影响。该模型较高的阴性预测值支持其在设计针对性淋巴水肿监测方案以进行早期干预中的应用。