Dipartimento di Scienze Biomediche Avanzate, Università FEDERICO II, Via S. Pansini N. 5, Naples, Italy.
UOC Cardiochirurgia Azienda Ospedaliera Universitaria FEDERICO II, Naples, Italy.
J Med Case Rep. 2024 Nov 7;18(1):524. doi: 10.1186/s13256-024-04884-7.
The complications associated with cardiac device implants ranges between 5.3% and 14.3%. Cardiac perforation due to "leads" represent a very rare complication of cardiac device implantation, ranging between 0.3% and 0.7%. Clinically, they can manifest different, nonspecific symptoms; hence, the diagnosis may not be immediate.
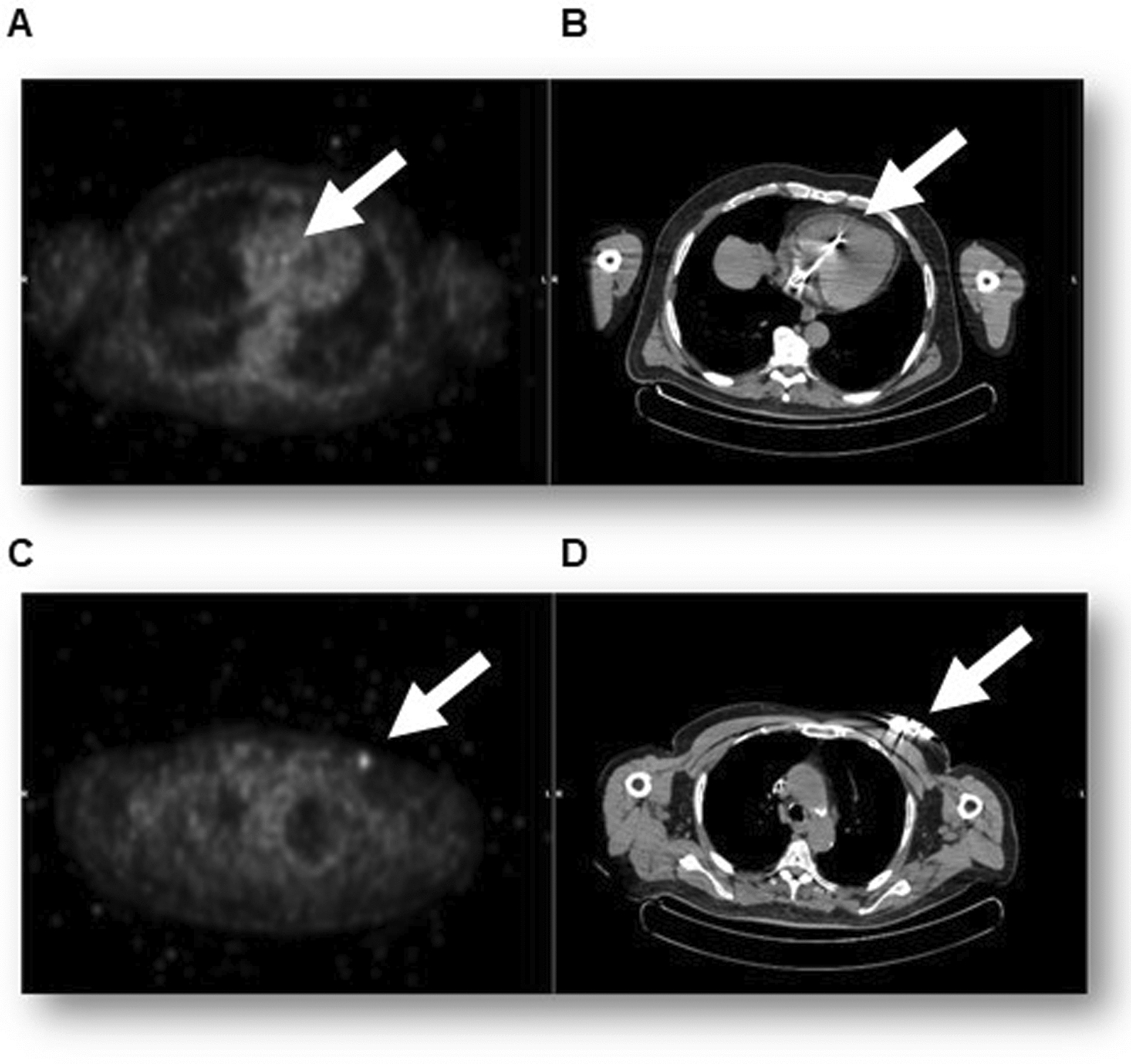
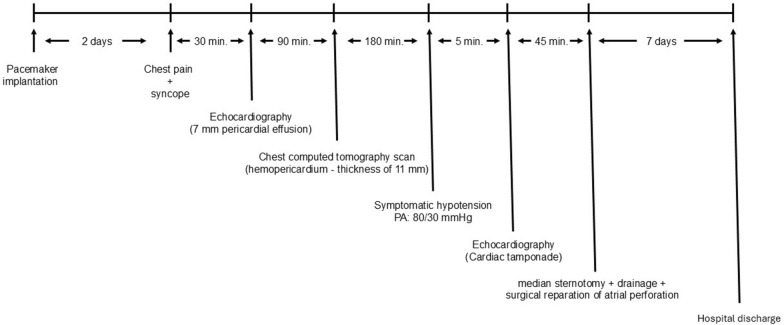
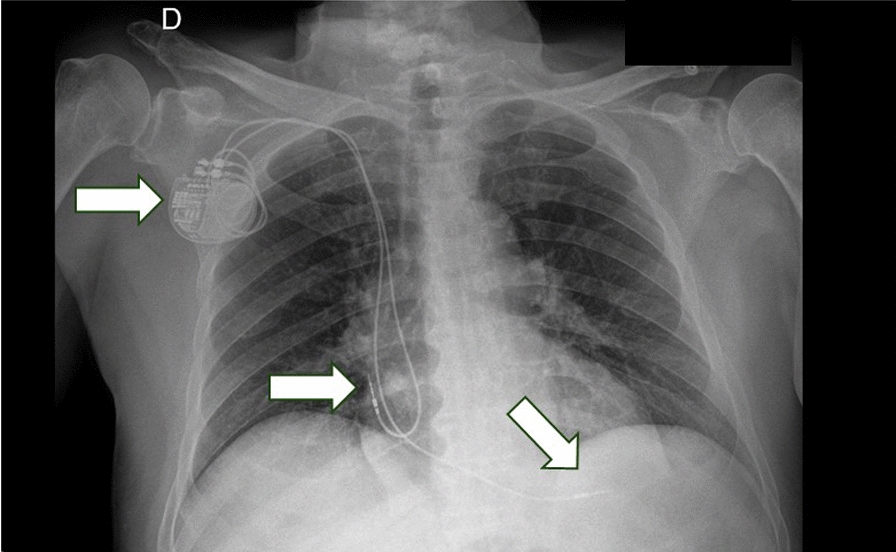
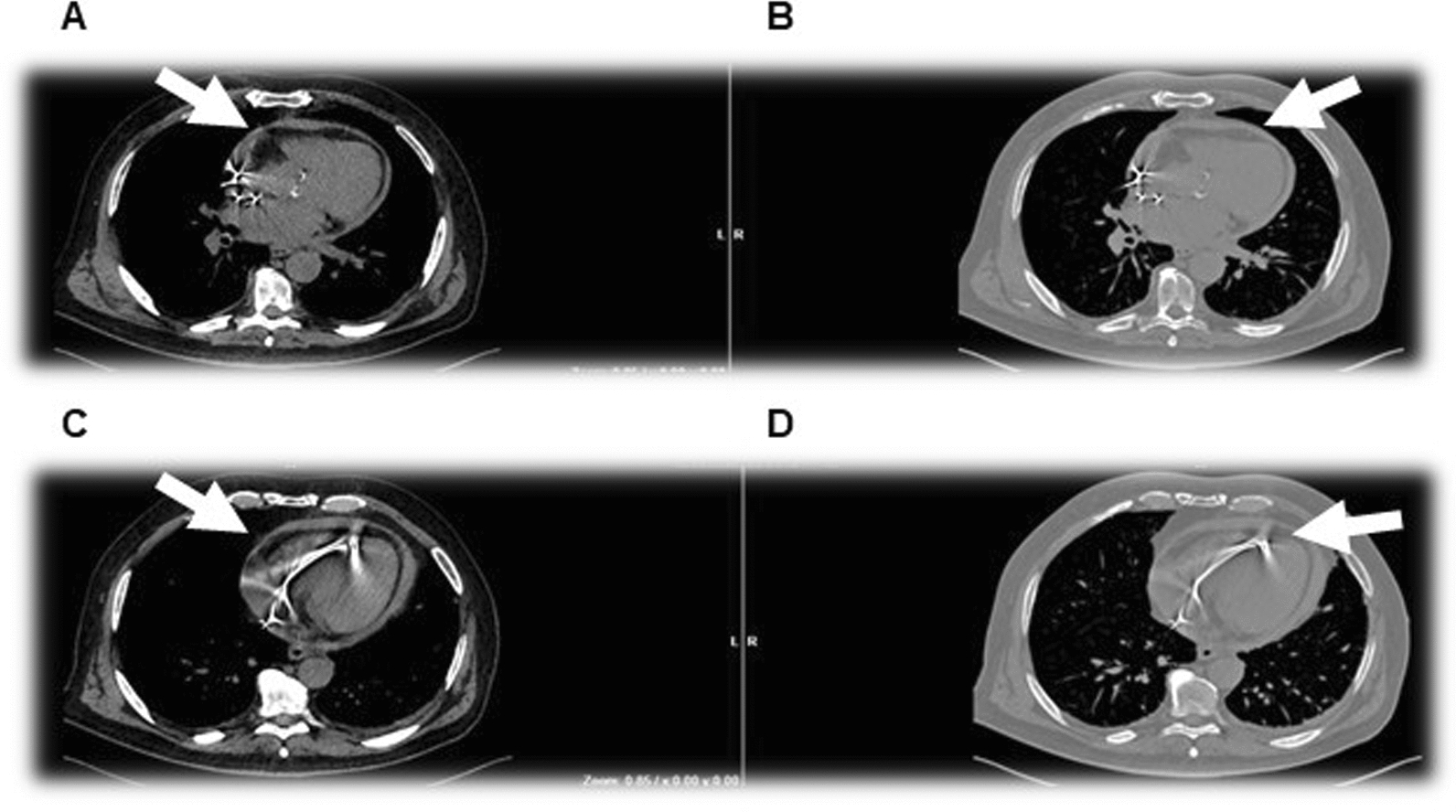
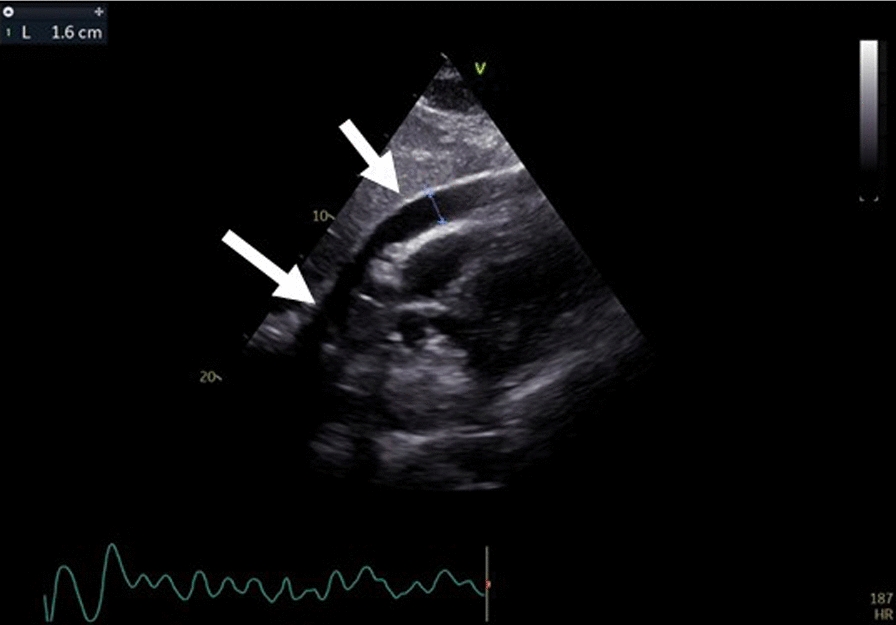
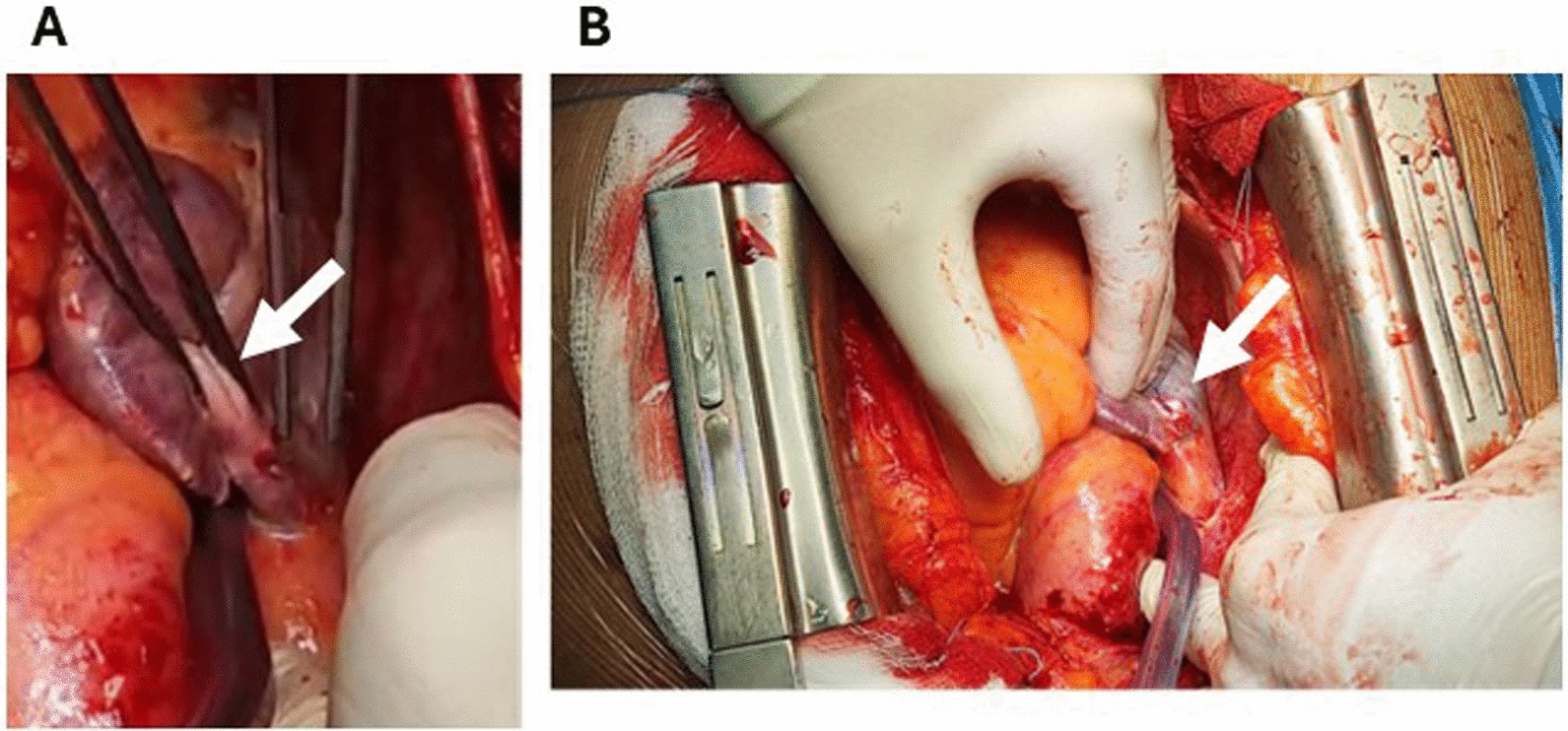
Our clinical case describes the successful treatment of cardiac tamponade occurring in a Caucasian 79-year-old man following a pacemaker implantation. Two days after the procedure, the patient reported an episode of nonspecific chest pain associated with syncope. The echocardiogram performed revealed a pericardial effusion in the apical area, along the right chambers, with a thickness of 7 mm, not hemodynamically significant. A chest computed tomography scan with contrast showed hemopericardium (maximum thickness of 11 mm), caused by an atrial perforation. A few hours later, the patient experienced hemodynamic instability. For this reason, an urgent sternotomy was performed with drainage of a significant hemopericardial effusion, revealing a perforation of the upper free wall of the right atrium with pericardial injury caused by the retractable screw lead. The perforation site was sutured and the sternal wound was closed. The patient was discharged after 4 days without further complications. At the control visit, scheduled 30 days after the hospital discharge, the patient was in good conditions.
Although the atrial perforations from leads are very rare complications of pacemaker implantation procedures, they are potentially lethal. In conclusion, this clinical case highlights the need, before hospital discharge, of an accurate screening for evaluation the pericardial effusion in patients that undergo to the cardiac implantable electronic devices.
心脏器械植入相关并发症发生率在 5.3%至 14.3%之间。心脏穿孔由“导联”引起,是心脏器械植入的一种非常罕见的并发症,发生率在 0.3%至 0.7%之间。临床上,它们可能表现为不同的、非特异性的症状;因此,诊断可能并不立即。
我们的临床病例描述了一名 79 岁白人男性在植入起搏器后发生心脏压塞的成功治疗。术后两天,患者报告出现非特异性胸痛伴晕厥。超声心动图显示心尖区和右心腔沿导联存在心包积液,厚度为 7mm,无血流动力学意义。胸部 CT 扫描显示存在血胸(最大厚度为 11mm),由心房穿孔引起。几小时后,患者出现血流动力学不稳定。因此,紧急进行了开胸术并引流大量血心包积液,发现可回收螺钉导联引起的右心房上壁穿孔和心包损伤。穿孔部位缝合,胸骨伤口关闭。患者在无进一步并发症的情况下于 4 天后出院。在出院后 30 天的随访时,患者情况良好。
尽管导联引起的心房穿孔是心脏起搏器植入术非常罕见的并发症,但它们可能是致命的。总之,这个临床病例强调了在患者出院前,需要对接受心脏植入电子设备的患者进行心包积液的准确筛查。