UPMC, Pittsburgh, Pennsylvania, USA.
Center for Clinical Neurophysiology, University of Pittsburgh Medical Center Health System, Pittsburgh, Pennsylvania, USA.
Open Heart. 2024 Nov 9;11(2):e002939. doi: 10.1136/openhrt-2024-002939.
To evaluate the impact of intraoperative neuromonitoring (IONM) on stroke and operative mortality after coronary and/or valvular operations.
This was an observational study of coronary and/or valvular heart operations from 2010 to 2021. Baseline characteristics and postoperative outcomes were compared by the use or non-use of IONM, which included both electroencephalography and somatosensory-evoked potentials. Propensity-score matching was employed to assess the association of IONM usage with operative mortality and stroke.
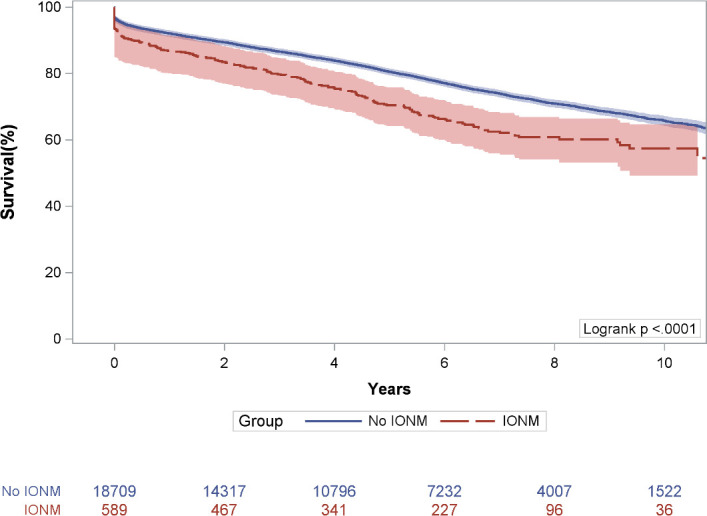
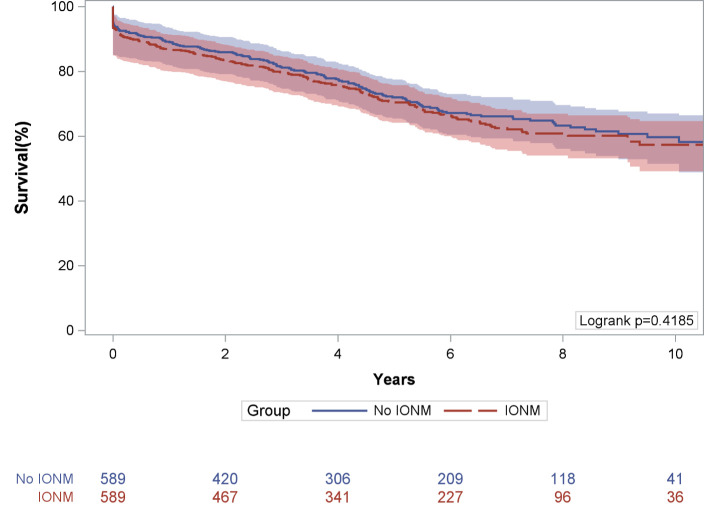
A total of 19 299 patients underwent a cardiac operation, of which 589 (3.1%) had IONM. Patients with IONM were more likely to have had baseline cerebrovascular disease (60% vs 22%). Patients with IONM had increased operative mortality (5.3% vs 2.5%) and stroke (4.9% vs 1.9%). Moreover, stroke and mortality were highly correlated, with 14% of strokes resulting in death, while only 2% of non-strokes resulted in death (p<0.001). The unadjusted Kaplan-Meier survival estimate was significantly lower among the group with IONM (p<0.001, log-rank). After propensity matching, however, there was no difference in operative mortality or stroke across each group: 3.6% vs 5.3% for mortality and 3.7% vs 5.4% for stroke. In the propensity-matched cohort, the Kaplan-Meier survival estimates were not significantly different across each group (p=0.419, log-rank).
Adjusting for baseline risk, there was no significant difference in adverse outcomes across each group. IONM may serve as a biomarker of cerebral ischaemia, and empirical adjustments based on changes may provide benefits for neurologic outcomes in high-risk patients. The efficacy of IONM during cardiac surgery should be prospectively validated.
评估术中神经监测(IONM)对冠状动脉和/或瓣膜手术后中风和手术死亡率的影响。
这是一项 2010 年至 2021 年冠状动脉和/或瓣膜心脏手术的观察性研究。通过使用或不使用 IONM(包括脑电图和体感诱发电位)比较基线特征和术后结果。采用倾向评分匹配评估 IONM 使用与手术死亡率和中风的关联。
共 19299 例患者接受了心脏手术,其中 589 例(3.1%)进行了 IONM。有 IONM 的患者更有可能患有基线脑血管疾病(60%比 22%)。有 IONM 的患者手术死亡率(5.3%比 2.5%)和中风(4.9%比 1.9%)更高。此外,中风和死亡率高度相关,14%的中风导致死亡,而只有 2%的非中风导致死亡(p<0.001)。IONM 组的未经调整的 Kaplan-Meier 生存估计明显较低(p<0.001,对数秩)。然而,在进行倾向评分匹配后,每组之间的手术死亡率或中风无差异:死亡率为 3.6%比 5.3%,中风为 3.7%比 5.4%。在倾向匹配队列中,每组之间的 Kaplan-Meier 生存估计没有显著差异(p=0.419,对数秩)。
调整基线风险后,每组的不良结局无显著差异。IONM 可能是脑缺血的生物标志物,基于变化的经验性调整可能为高危患者的神经结局带来益处。IONM 在心脏手术中的疗效应进行前瞻性验证。