Freedland Stephen J, Fernandes Luis, De Solda Francesco, Buyukkaramikli Nasuh, Mundle Suneel D, McCarthy Sharon A, Labson Daniel, Yang Lingfeng, Pan Feng, Mir Carmen
Cedars-Sinai Medical Center, Samuel Oschin Comprehensive Cancer Institute, Los Angeles, CA, USA.
Durham VA Medical Center, Durham, NC, USA.
Target Oncol. 2025 Jan;20(1):139-148. doi: 10.1007/s11523-024-01113-5. Epub 2024 Nov 10.
Patients with high-risk localized and locally advanced prostate cancer (HR-LPC/LAPC) have increased risk of metastasis, leading to reduced survival rates. Segmenting the disease course [time to recurrence, recurrence to metastasis, and post-metastasis survival (PMS)] may identify disease states for which the greatest impacts can be made to ultimately improve survival.
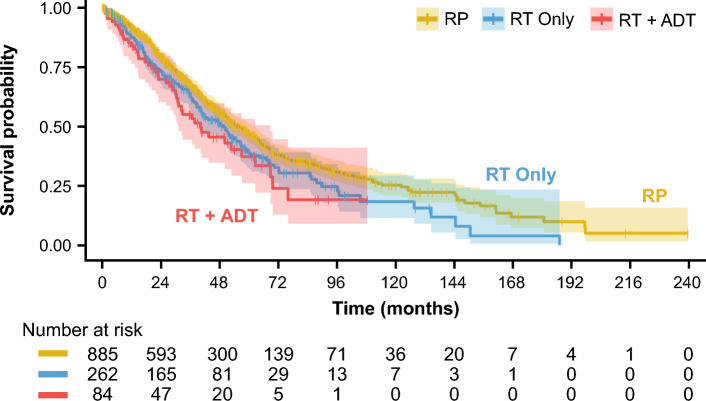
Evaluate real-world PMS of patients with HR-LPC/LAPC who received primary radical prostatectomy (RP) or radiotherapy (RT) with or without androgen deprivation therapy (ADT).
Electronic health records from an oncology database were used to assess PMS. Risk of death was estimated using the Kaplan-Meier method. Hazard ratios (HRs) were used to analyze the impact of treatment and time to metastasis (TTM) on PMS. Standardized mortality ratios (SMRs) were calculated for patients with HR-LPC/LAPC versus the US general male population.
Overall, 5008 patients with HR-LPC/LAPC were identified, and 1231 developed metastases after primary treatment (RP, n = 885; RT only, n = 262; RT+ADT, n = 84). Age-adjusted PMS HR between the RP and RT only cohorts was 1.19 (p = 0.077) and between RP and RT+ADT cohorts was 1.32 (p = 0.078). TTM was unrelated to PMS in unadjusted (HR 1.01, p = 0.2) and age-adjusted models (HR 0.99, p = 0.3). Relative to pre-metastasis SMRs, post-metastasis SMRs increased eightfold and fivefold in patients treated with RP and RT±ADT, respectively.
PMS was unrelated to TTM in patients with HR-LPC/LAPC, suggesting PMS may be independent of the trajectory to development of metastases. Given PMS may be a fixed length of time, delaying the development of metastasis may improve survival in patients with HR-LPC/LAPC.
高危局限性和局部晚期前列腺癌(HR-LPC/LAPC)患者发生转移的风险增加,导致生存率降低。对疾病进程进行分段[复发时间、复发至转移时间以及转移后生存期(PMS)]可能会确定那些对最终提高生存率影响最大的疾病状态。
评估接受原发性根治性前列腺切除术(RP)或放疗(RT)联合或不联合雄激素剥夺治疗(ADT)的HR-LPC/LAPC患者的真实世界PMS。
使用肿瘤数据库中的电子健康记录来评估PMS。采用Kaplan-Meier方法估计死亡风险。使用风险比(HR)分析治疗和转移时间(TTM)对PMS的影响。计算HR-LPC/LAPC患者与美国普通男性人群的标准化死亡比(SMR)。
总体而言,共识别出5008例HR-LPC/LAPC患者,其中1231例在初始治疗后发生转移(RP组,n = 885;单纯RT组,n = 262;RT + ADT组,n = 84)。RP组与单纯RT组之间经年龄调整的PMS HR为1.19(p = 0.077),RP组与RT + ADT组之间为1.32(p = 0.078)。在未调整模型(HR 1.01,p = 0.2)和年龄调整模型(HR 0.99,p = 0.3)中,TTM与PMS无关。相对于转移前SMR,接受RP治疗和RT±ADT治疗的患者转移后SMR分别增加了8倍和5倍。
HR-LPC/LAPC患者的PMS与TTM无关,提示PMS可能独立于转移发生轨迹。鉴于PMS可能是一段固定时间,延迟转移的发生可能会提高HR-LPC/LAPC患者的生存率。