Department of Neurosurgery. 020021, University of Medicine and Pharmacy "Carol Davila", Bucharest, Romania.
Neurosurgical Department, . Pantelimon Emergency Hospital, Bucharest, Romania.
Neurosurg Rev. 2024 Nov 11;47(1):841. doi: 10.1007/s10143-024-03088-3.
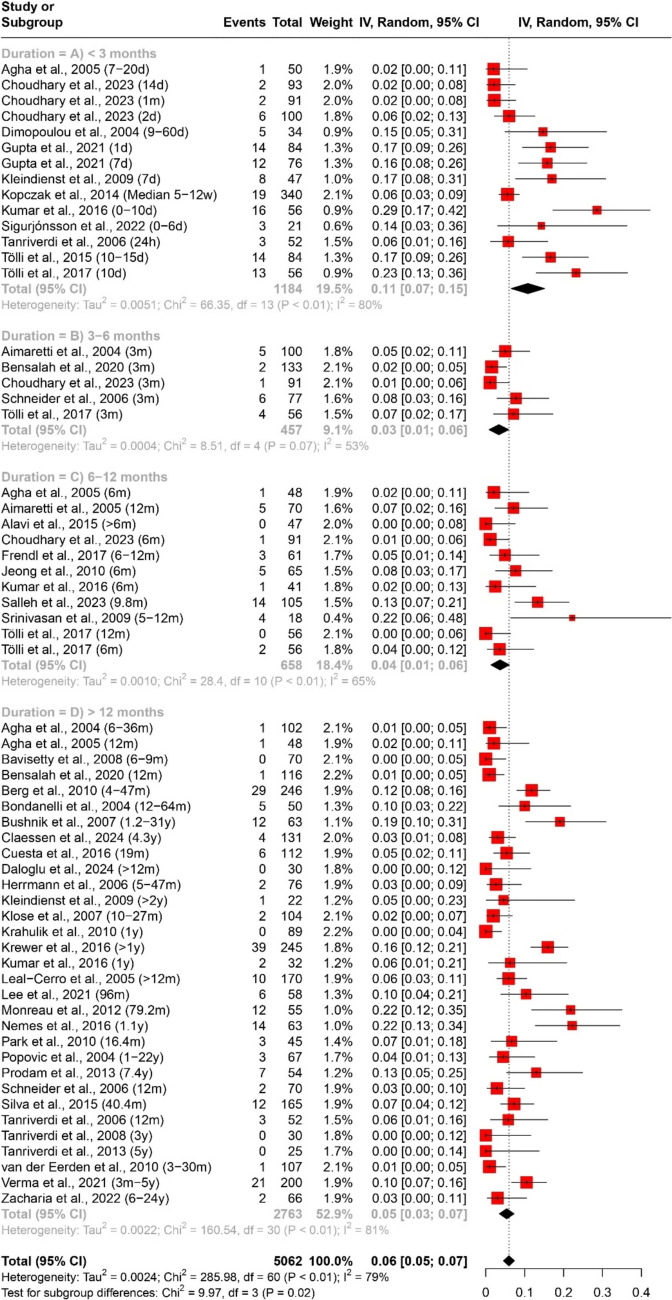
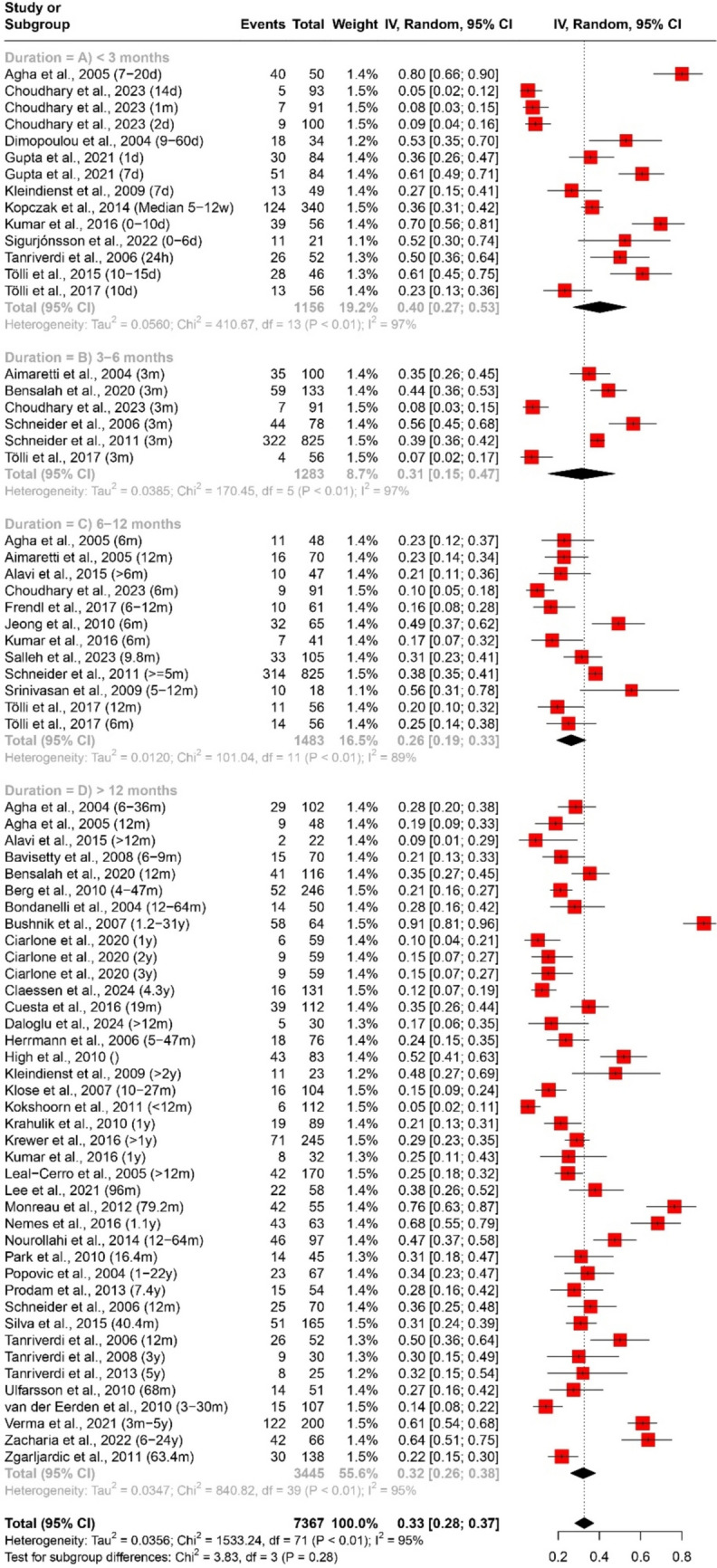
Traumatic brain injury (TBI) is associated with various endocrine abnormalities, including pituitary axis dysfunction. Understanding the prevalence and temporal patterns of these dysfunctions is crucial for effective clinical management. This study aimed to systematically review the literature and conduct a meta-analysis to determine the prevalence of pituitary axis dysfunction following TBI, assess temporal patterns across different post-injury durations, and identify potential contributing factors. A comprehensive search was conducted across multiple electronic databases between 1st of January 2000 until 31st March 2024. Studies reporting the prevalence of pituitary axis dysfunction post-TBI were included. Pooled estimates with 95% confidence intervals (CIs) were calculated using random-effects models in the R statistical software. Subgroup analyses were performed based on duration post-TBI (< 3 months, 3-6 months, 6-12 months, > 12 months) to explore temporal variations. Heterogeneity was assessed using the I^2 statistic. A total of 52 studies were included in the meta-analysis, encompassing 7367 participants. The pooled estimate for the prevalence of any pituitary axis dysfunction post-TBI was 33% (95% CI [28%; 37%]). Subgroup analysis by duration revealed varying prevalence rates: < 3 months (40%, 95% CI [27%; 53%]), 3-6 months (31%, 95% CI [15%; 47%]), 6-12 months (26%, 95% CI [19%; 33%]), and > 12 months (32%, 95% CI [26%; 38%]). Prevalence of multiple axes affection was 7% (95% CI [6%; 9%]), with varying rates across durations. Specific axes affection varied: Growth Hormone (GH) deficiency was 18% (95% CI [14%; 21%]), adrenocorticotropic hormone (ACTH) deficiency was 10% (95% CI [8%; 13%]), pituitary-gonadal axis hormones deficiency was 16% (95% CI [12%; 19%]), and thyroid-stimulating hormone (TSH) deficiency was 6% (95% CI [5%; 7%]). This meta-analysis highlights a significant prevalence of pituitary axis dysfunction following TBI, with temporal variations observed across different post-injury durations. The findings underscore the importance of tailored clinical management strategies based on the duration and type of dysfunction. Further research addressing potential contributing factors is warranted to enhance understanding and management of these conditions.
创伤性脑损伤(TBI)与各种内分泌异常有关,包括垂体轴功能障碍。了解这些功能障碍的患病率和时间模式对于有效的临床管理至关重要。本研究旨在系统地回顾文献并进行荟萃分析,以确定 TBI 后垂体轴功能障碍的患病率,评估不同损伤后时间的时间模式,并确定潜在的促成因素。在 2000 年 1 月 1 日至 2024 年 3 月 31 日期间,在多个电子数据库中进行了全面搜索。纳入了报告 TBI 后垂体轴功能障碍患病率的研究。使用 R 统计软件中的随机效应模型计算了具有 95%置信区间(CI)的汇总估计值。根据损伤后时间(<3 个月、3-6 个月、6-12 个月、>12 个月)进行亚组分析,以探讨时间变化。使用 I^2 统计量评估异质性。荟萃分析共纳入 52 项研究,包含 7367 名参与者。TBI 后任何垂体轴功能障碍的总体患病率为 33%(95%CI[28%;37%])。按时间进行的亚组分析显示出不同的患病率:<3 个月(40%,95%CI[27%;53%])、3-6 个月(31%,95%CI[15%;47%])、6-12 个月(26%,95%CI[19%;33%])和>12 个月(32%,95%CI[26%;38%])。多个轴受累的患病率为 7%(95%CI[6%;9%]),不同时间的患病率不同。特定轴受累情况有所不同:生长激素(GH)缺乏症为 18%(95%CI[14%;21%]),促肾上腺皮质激素(ACTH)缺乏症为 10%(95%CI[8%;13%]),垂体性腺轴激素缺乏症为 16%(95%CI[12%;19%]),促甲状腺激素(TSH)缺乏症为 6%(95%CI[5%;7%])。这项荟萃分析强调了 TBI 后垂体轴功能障碍的显著患病率,并观察到不同损伤后时间的时间变化。研究结果强调了根据功能障碍的持续时间和类型制定量身定制的临床管理策略的重要性。需要进一步研究潜在促成因素,以提高对这些情况的认识和管理。