Luo Xu-Ying, Zhou Yi-Min, Zhou Jianfang, He Xuan, Chen Guang-Qiang, Li Hong-Liang, Yang Yan-Lin, Zhang Linlin, Zhou Jian-Xin
Department of Critical Care Medicine, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
Department of Critical Care Medicine, Beijing Shijitan Hospital, Capital Medical University, Beijing, China.
J Thorac Dis. 2024 Oct 31;16(10):6441-6451. doi: 10.21037/jtd-24-694. Epub 2024 Oct 30.
Reverse triggering (RT) is a ventilatory asynchrony characterized by the activation of respiratory muscles in response to passive mechanical insufflation. Although RT can potentially exacerbate lung injury, its characteristics in patients with acute brain injury remain under-explored. This study aims to elucidate the incidence and factors associated with RT in this patient population.
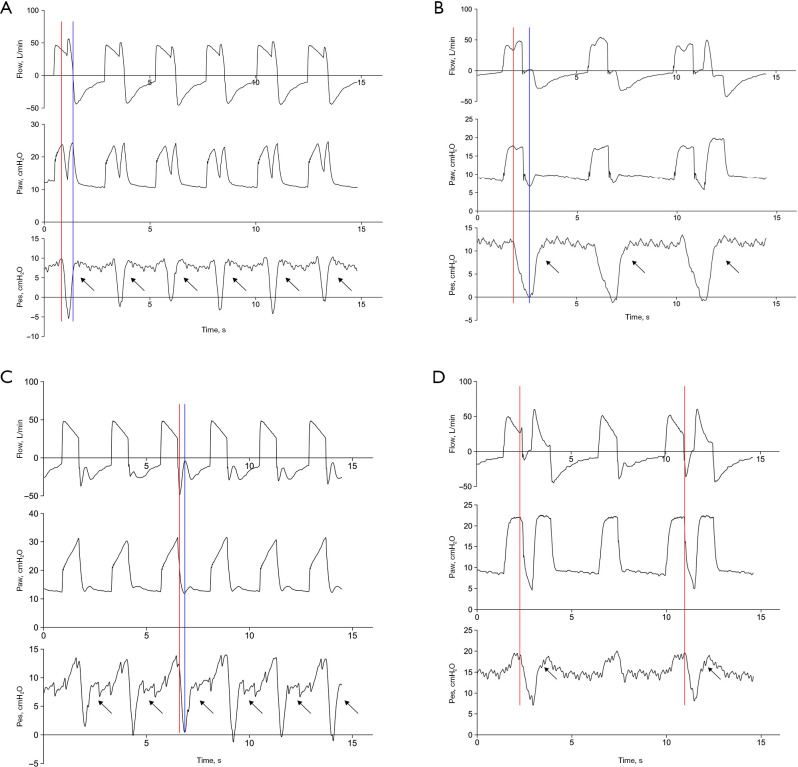
A retrospective analysis was conducted using a clinical database dedicated to investigating patient-ventilator asynchrony among individuals with acute brain injury. Only patients under controlled mechanical ventilation were included. RT was identified through an analysis of airway pressure, flow, and esophageal pressure waveforms collected at 15-minute intervals. The incidence of RT was determined by calculating the ratio of the number of RT breaths to the total number of breaths.
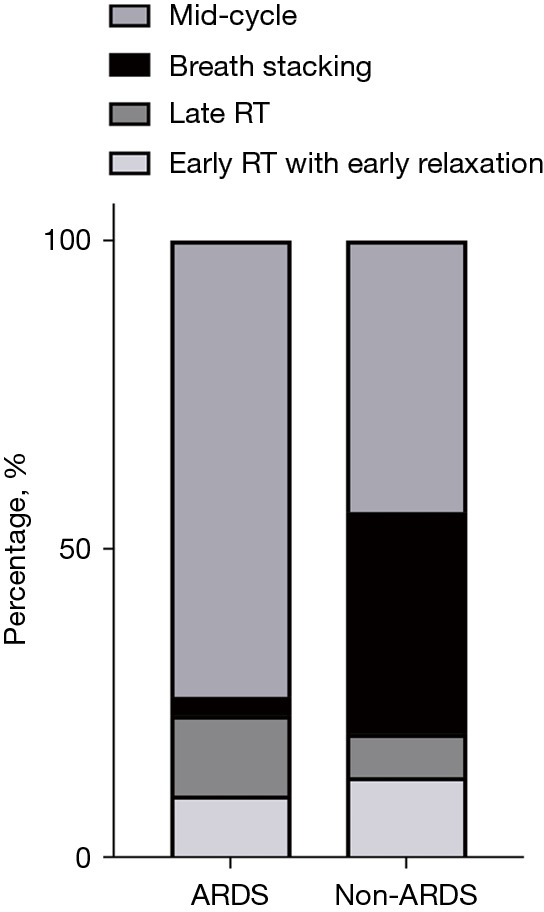
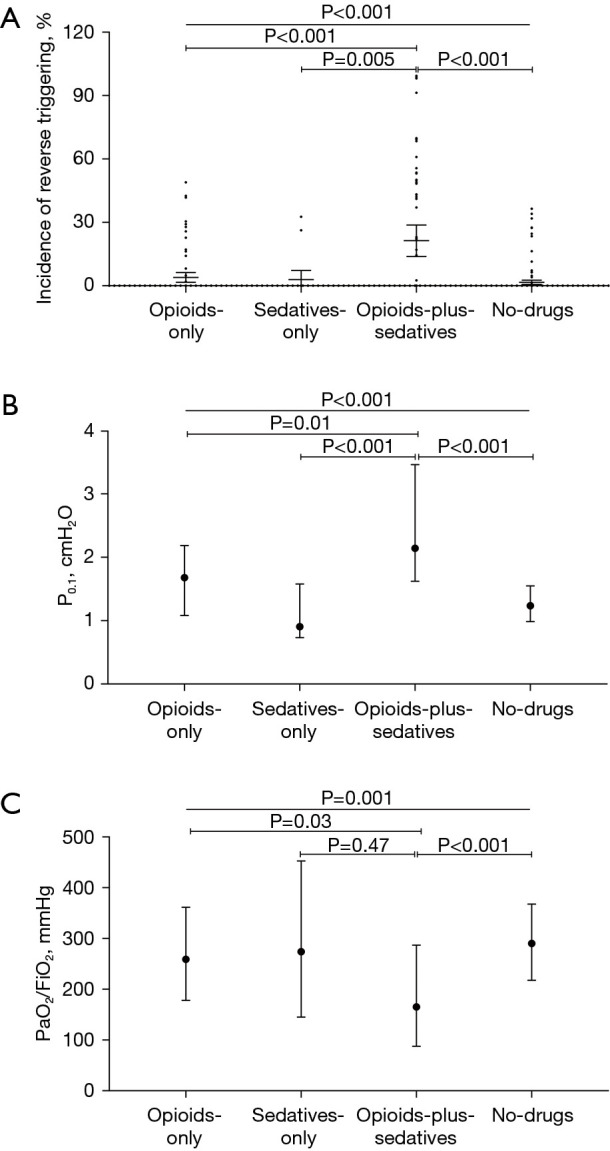
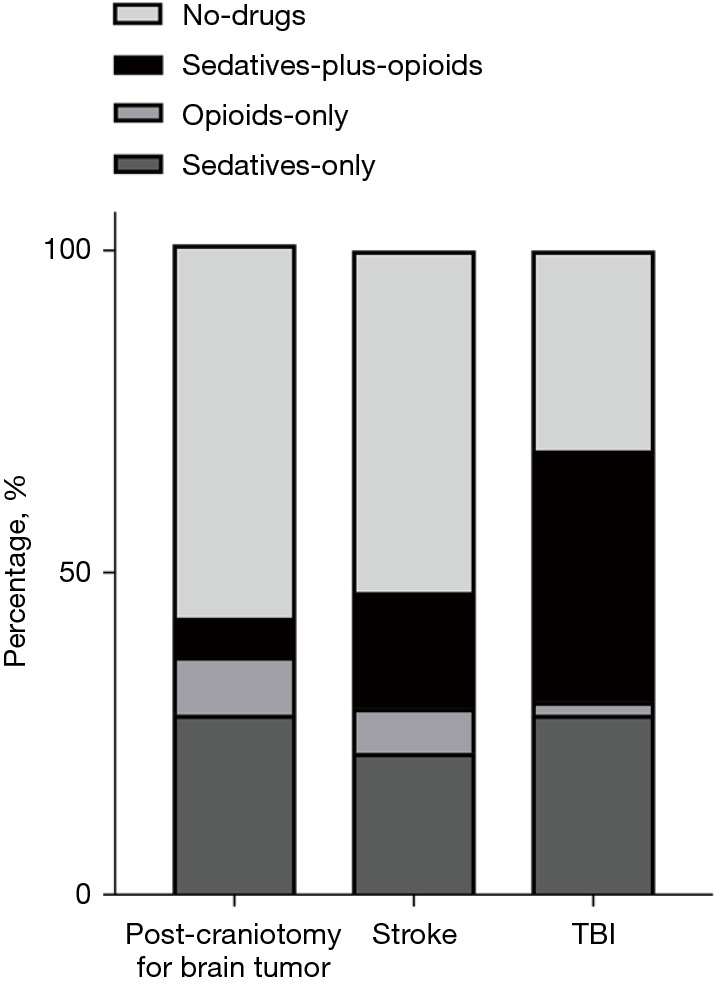
A total of 334 waveform datasets from 53 patients were analyzed. RT was observed in 8.4% of mechanical insufflations across 59 datasets (17.7%). Sixteen patients (30.2%) experienced at least one RT event. The most prevalent phenotype was mid-cycle RT (61.1%), followed by breath stacking (BD) (16.6%). Independent predictors of RT, after adjusting for confounding factors, included the combined use of opioids and sedatives, lower Sedation-Agitation Scale (SAS) scores, reduced airway delta pressure, and minimal discrepancies between the set respiratory rate and the actual respiratory rate. The pressure of occlusion at 0.1 seconds (P) demonstrated substantial predictive ability for BD, with an area under the receiver operating characteristics curve of 0.72 (95% confidence interval: 0.64-0.80, P<0.001); the optimal cutoff was determined to be 1.69 cmHO, achieving 83.3% sensitivity and 67.1% specificity.
Factors such as deep sedation, lower airway delta pressure, and close alignment of ventilator and patient respiratory rates were associated with RT in patients with acute brain injury. Additionally, P served as a reliable predictor for the occurrence of BD.
反向触发(RT)是一种通气不同步现象,其特征是呼吸肌对被动机械通气产生反应而激活。尽管RT可能会加重肺损伤,但其在急性脑损伤患者中的特征仍未得到充分研究。本研究旨在阐明该患者群体中RT的发生率及相关因素。
使用一个专门用于调查急性脑损伤患者呼吸机不同步情况的临床数据库进行回顾性分析。仅纳入接受控制机械通气的患者。通过分析每隔15分钟收集的气道压力、流量和食管压力波形来识别RT。RT的发生率通过计算RT呼吸次数与总呼吸次数的比值来确定。
共分析了来自53例患者的334个波形数据集。在59个数据集中(17.7%),8.4%的机械通气观察到了RT。16例患者(30.2%)经历了至少一次RT事件。最常见的表型是周期中RT(61.1%),其次是呼吸叠加(BD)(16.6%)。在调整混杂因素后,RT的独立预测因素包括阿片类药物和镇静剂的联合使用、较低的镇静-躁动评分(SAS)、气道压差降低以及设定呼吸频率与实际呼吸频率之间的最小差异。0.1秒时的闭塞压力(P)对BD具有显著的预测能力,受试者操作特征曲线下面积为0.72(95%置信区间:0.64 - 0.80,P<0.001);确定最佳截断值为1.69 cmH₂O,灵敏度为83.3%,特异性为67.1%。
深度镇静、较低的气道压差以及呼吸机与患者呼吸频率的紧密匹配等因素与急性脑损伤患者的RT相关。此外,P可作为BD发生的可靠预测指标。