Russell Nigel H, Thomas Abin, Hills Robert K, Thomas Ian, Gilkes Amanda, Almuina Nuria Marquez, Burns Sarah, Marsh Lucy, Vyas Paresh, Metzner Marlen, McCarthy Nicholas, Andrew Georgia, Byrne Jennifer, Sellar Rob S, Kelly Richard, Cahalin Paul, Overgaard Ulrik Malthe, Mehta Priyanka, Dennis Mike, Knapper Steven, Freeman Sylvie D
Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom.
Centre for Trials Research, Cardiff University, Cardiff, United Kingdom.
J Clin Oncol. 2025 Feb 20;43(6):694-704. doi: 10.1200/JCO.24.00259. Epub 2024 Nov 18.
To evaluate the survival benefit of chemotherapy intensification in older patients with AML who have not achieved a measurable residual disease (MRD)-negative remission.
Five hundred twenty-three patients with AML (median age, 67 years; range, 51-79) without a flow cytometric MRD-negative remission response after a first course of daunorubicin and AraC (DA; including 165 not in remission) were randomly assigned between up to two further courses of DA or intensified chemotherapy-either fludarabine, cytarabine, granulocyte colony-stimulating factor and idarubicin (FLAG-Ida) or DA with cladribine (DAC).
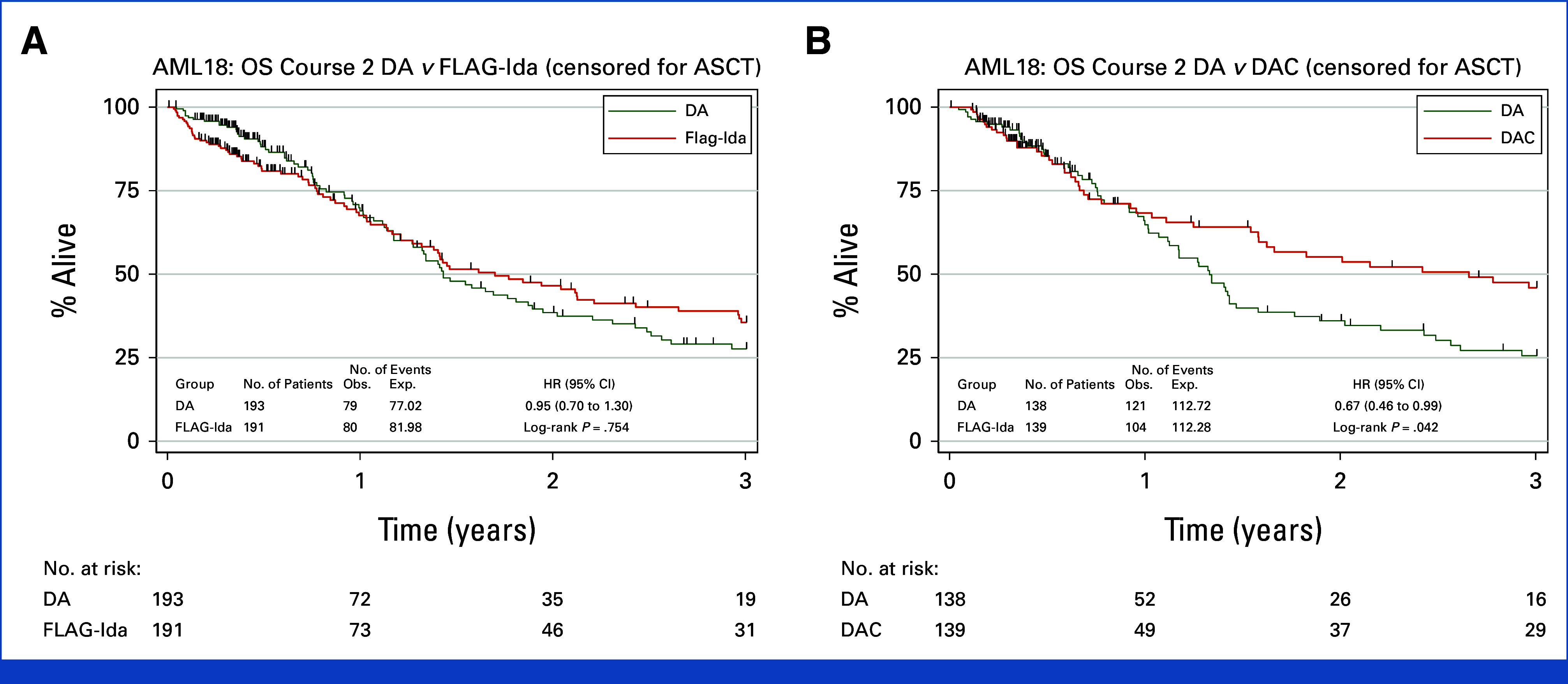
Overall survival (OS) was not improved in the intensification arms (DAC DA: hazard ratio [HR], 0.74 [95% CI, 0.55 to 1.01]; = .054; FLAG-Ida DA: HR, 0.86 [95% CI, 0.66 to 1.12]; = .270); OS at 3 years was 34%, 46%, and 42% for DA, DAC, and FLAG-Ida, respectively. Early deaths and other adverse events were more frequent with FLAG-Ida (9% day 60 deaths 4% after DA or DAC; = .032). Of patients entering random assignment, 131 had MRD unknown status. In this subgroup of patients lacking evidence of residual leukemia by flow cytometry, there was no detectable survival advantage from intensification. A planned sensitivity analysis excluding these patients demonstrated a survival benefit for both DAC (HR, 0.66 [95% CI, 0.46 to 0.93]; = .018) and FLAG-Ida (HR, 0.72 [95% CI, 0.53 to 0.98]; = .035); OS at 3 years was 30%, 46%, and 46% for DA, DAC, and FLAG-Ida, respectively. There was a concordant reduction in relapse (DAC DA: HR, 0.66 [95% CI, 0.45 to 0.98]; = .039; FLAG-Ida DA: HR, 0.70 [95% CI, 0.49 to 0.99]; = .042). DAC benefit was maintained when survival was censored for transplant ( = .042).
In this study of older patients with AML considered fit and with evidence of residual disease after first induction, chemotherapy intensification improved survival. DAC intensification was better tolerated than FLAG-Ida.
评估强化化疗对未达到可测量残留病(MRD)阴性缓解的老年急性髓系白血病(AML)患者的生存获益。
523例AML患者(中位年龄67岁;范围51 - 79岁),在接受柔红霉素和阿糖胞苷(DA)的第一个疗程后未获得流式细胞术MRD阴性缓解反应(包括165例未缓解患者),被随机分配接受至多两个额外疗程的DA或强化化疗,即氟达拉滨、阿糖胞苷、粒细胞集落刺激因子和伊达比星(FLAG - Ida)或DA联合克拉屈滨(DAC)。
强化化疗组的总生存期(OS)未得到改善(DAC vs DA:风险比[HR],0.74[95%CI,0.55至1.01];P = 0.054;FLAG - Ida vs DA:HR,0.86[95%CI,0.66至1.12];P = 0.270);DA、DAC和FLAG - Ida组3年OS分别为34%、46%和42%。FLAG - Ida组早期死亡和其他不良事件更频繁(60天死亡率9% vs DA或DAC后的4%;P = 0.032)。进入随机分组的患者中,131例MRD状态未知。在这个通过流式细胞术缺乏残留白血病证据的患者亚组中,强化化疗未显示出可检测到的生存优势。一项排除这些患者的计划敏感性分析显示DAC(HR,0.66[95%CI,0.46至0.93];P = 0.018)和FLAG - Ida(HR,0.72[95%CI,0.53至0.98];P = 0.035)均有生存获益;DA、DAC和FLAG - Ida组3年OS分别为30%、46%和46%。复发率有相应降低(DAC vs DA:HR,0.66[95%CI,0.45至0.98];P = 0.039;FLAG - Ida vs DA:HR,0.70[95%CI,0.49至0.99];P = 0.042)。当对移植进行生存审查时,DAC的获益得以维持(P = 0.042)。
在这项针对被认为适合且首次诱导后有残留病证据的老年AML患者的研究中,强化化疗改善了生存。DAC强化化疗的耐受性优于FLAG - Ida。