Agarwal Sanjay K, Stokes Michael, Chen Rong, Lickert Cassandra
Gynecology, and Reproductive Sciences, University of California San Diego, La Jolla, CA (Agarwal).
Evidera, St. Laurent, Quebec, Canada (Stokes).
AJOG Glob Rep. 2024 Oct 17;4(4):100412. doi: 10.1016/j.xagr.2024.100412. eCollection 2024 Nov.
Historically, the clinical characteristics and treatment pathways for patients with uterine fibroids and heavy menstrual bleeding have differed between White and Black women.
To provide a contemporary comparison of patient characteristics and treatment patterns among White and Black women with uterine fibroids and heavy menstrual bleeding in the United States.
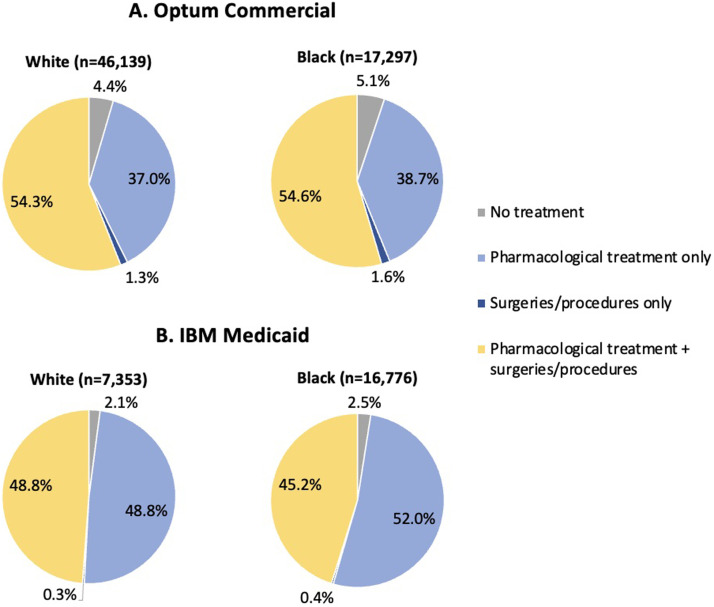
This retrospective cohort study included administrative claims data from 46,139 White and 17,297 Black women with uterine fibroids and heavy menstrual bleeding from the Optum Clinformatics database (January 2011-December 2020) and 7353 White and 16,776 Black women from the IBM MarketScan Multi-State Medicaid Insurance database (January 2010-December 2019). Patients were indexed at their initial uterine fibroid diagnosis claim and were required to have a claim for heavy menstrual bleeding and ≥12 months of continuous enrollment pre- and postindex. Patients were followed until the earliest of death, disenrollment, hysterectomy date, or end of study database. Outcomes were stratified by race and included patient demographics, clinical characteristics, pharmacologic treatment patterns, and surgeries/procedures. Pearson's Chi-square test for categorical variables and Student's t-test for continuous data were used to evaluate differences in baseline characteristics. Descriptive statistics were used to characterize treatment pathways for hormonal contraceptive use in women with ≥24 months of follow-up. Kaplan-Meier survival analysis was used to estimate time until hysterectomy, with log-rank testing to assess between-group differences.
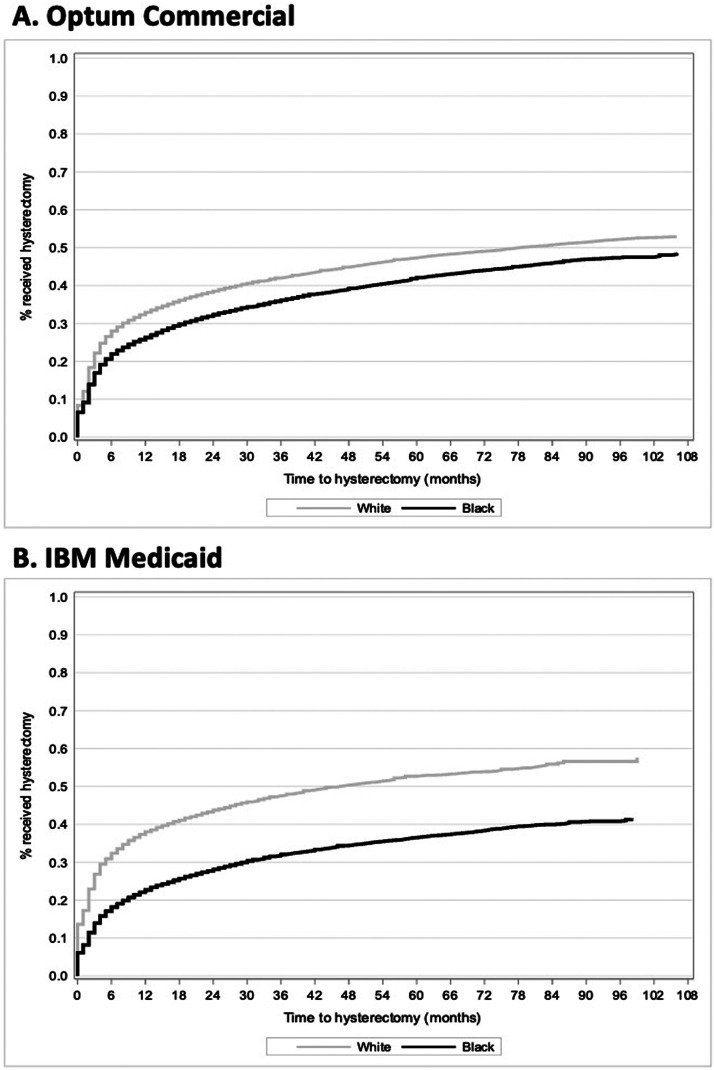
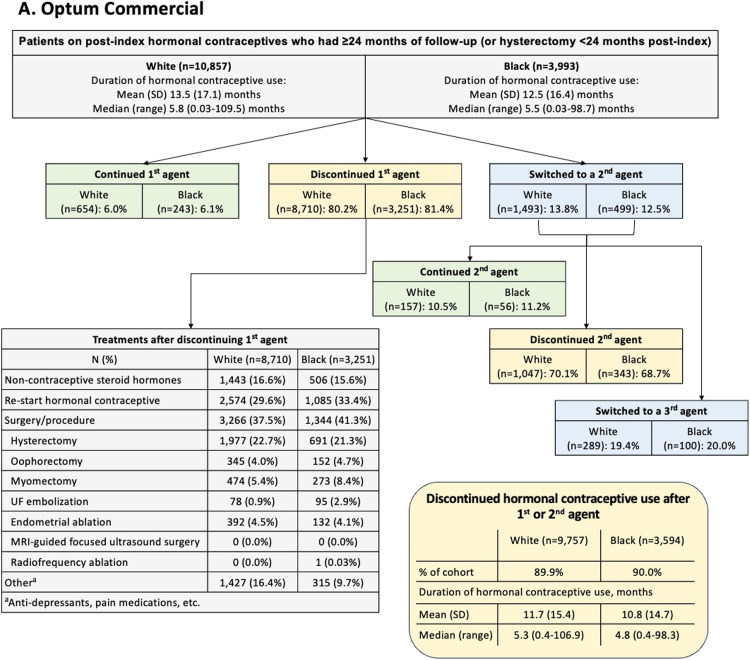
The mean (standard deviation) duration of follow-up was 44.6 (27.9) and 41.0 (24.9) months in the commercial and Medicaid databases, respectively. Mean (standard deviation) age at uterine fibroid diagnosis was lower for Black than White women in both databases (commercial: 42.3 [6.5] vs 44.4 [6.3] years; <.0001; Medicaid: 39.6 [7.1] years vs 40.2 [7.2] years; <.0001). Anemia was more prevalent in Black vs White women in both databases (commercial: 5.9% [1028/17,297] vs 3.6% [1648/46,139]; <.0001; Medicaid: 7.0% [1180/16,776] vs 4.5% [331/7353]; <.0001). In the commercial database, approximately one-half of women had claims for ≥1 bulk symptom, with no significant differences between groups. In the Medicaid database, significantly more White than Black women had claims for bulk symptoms (77.0% [5665/7353] vs 68.4% [11,477/16,776]; <.0001). Approximately 40% of all patients received hormonal drug therapies as initial treatment, most commonly hormonal contraceptives. However, discontinuation of hormonal contraceptive therapy was nearly universal, with one-half discontinuing within a median treatment duration of ∼5 months. Most women stopped treatment after 1 or 2 agents (commercial: White, 89.9% [9757/10,857]; Black, 90.0% [3594/3993]; Medicaid: White, 92.2% [1635/1773]; Black, 94.2% [4454/4726]). Hysterectomy was the most common procedure, and was more common among White vs Black women (commercial: 43.9% [20,235/46,139] vs 37.8% [6536/17,297]; Medicaid: 46.8% [3444/7353] vs 32.0% [5364/16,776]).
Black women with UF-HMB were diagnosed at a younger age than White women, and White women had higher hysterectomy rates than Black women, representing a shift from earlier researched treatment patterns. Patients with UF-HMB were also highly reliant on hormonal contraceptives, followed by nearly universal therapeutic discontinuation.
从历史上看,患有子宫肌瘤和月经过多的白人和黑人女性的临床特征及治疗途径有所不同。
对美国患有子宫肌瘤和月经过多的白人和黑人女性的患者特征及治疗模式进行当代比较。
这项回顾性队列研究纳入了Optum临床信息数据库(2011年1月至2020年12月)中46139名患有子宫肌瘤和月经过多的白人女性及17297名黑人女性,以及IBM MarketScan多州医疗补助保险数据库(2010年1月至2019年12月)中7353名白人女性和16776名黑人女性的行政索赔数据。患者以其最初的子宫肌瘤诊断索赔为索引,且要求在索引前后有月经过多的索赔记录以及连续参保≥12个月。对患者进行随访,直至最早出现死亡、退出参保、子宫切除日期或研究数据库结束。结果按种族分层,包括患者人口统计学特征、临床特征、药物治疗模式以及手术/操作。使用Pearson卡方检验分析分类变量,使用Student t检验分析连续数据,以评估基线特征的差异。使用描述性统计来描述随访≥24个月的女性使用激素避孕的治疗途径。采用Kaplan-Meier生存分析来估计直至子宫切除的时间,并使用对数秩检验评估组间差异。
在商业数据库和医疗补助数据库中,随访的平均(标准差)时长分别为44.6(27.9)个月和41.0(24.9)个月。在两个数据库中,黑人女性子宫肌瘤诊断时的平均(标准差)年龄均低于白人女性(商业数据库:42.3 [6.5]岁对44.4 [6.3]岁;P<0.0001;医疗补助数据库:39.6 [7.1]岁对40.2 [7.2]岁;P<0.0001)。在两个数据库中,贫血在黑人女性中比白人女性更普遍(商业数据库:5.9% [1028/17297]对3.6% [1648/46139];P<0.0001;医疗补助数据库:7.0% [1180/16776]对4.5% [331/7353];P<0.0001)。在商业数据库中,约一半的女性有≥1种主要症状的索赔记录,两组之间无显著差异。在医疗补助数据库中,有主要症状索赔记录的白人女性明显多于黑人女性(77.0% [5665/7353]对68.4% [11477/16776];P<0.0001)。约40%的所有患者接受激素药物治疗作为初始治疗,最常用的是激素避孕药。然而,激素避孕治疗的停药情况几乎很普遍,约一半的患者在中位治疗时长约5个月内停药。大多数女性在使用1或2种药物后停止治疗(商业数据库:白人,89.9% [9757/10857];黑人,90.0% [3594/3993];医疗补助数据库:白人,92.2% [1635/1773];黑人,94.2% [4454/4726])。子宫切除术是最常见的手术,在白人女性中比黑人女性更常见(商业数据库:43.9% [20235/46139]对37.8% [6536/17297];医疗补助数据库:46.8% [3444/7353]对32.0% [5364/16776])。
患有子宫肌瘤合并月经过多的黑人女性比白人女性诊断年龄更小,白人女性的子宫切除率高于黑人女性,这与早期研究的治疗模式有所不同。患有子宫肌瘤合并月经过多的患者也高度依赖激素避孕药,随后几乎普遍停药。