Luque Paz Damien, Gagelmann Nico, Benajiba Lina, Riou Jérémie, Salit Rachel, Orvain Corentin, Schroeder Thomas, Bories Claire, Gurnari Carmelo, Badbaran Anita, Boyer Françoise, Pagliuca Simona, Rautenberg Christina, Tavitian Suzanne, Pangiota Victoria, Ianotto Jean-Christophe, Thol Felicitas, Cayssials Emilie, Heuser Michael, Rubio Marie-Thérèse, Cassinat Bruno, Daltro de Oliveira Rafael, Sauter Craig, Maciejewski Jaroslaw P, Reinhardt Hans Christian, Scott Bart L, Ugo Valérie, Kröger Nicolaus, Kiladjian Jean-Jacques, Robin Marie
Laboratoire d'hématologie, Université Angers, Nantes Université, CHU Angers, INSERM, CNRS, CRCI2NA, F-49000, Angers, France.
Fédération Hospitalo Universitaire Grand-Ouest Acute Leukemia, FHU-GOAL and Université d'Angers, INSERM UMR 1307, CNRS UMR 6075, Nantes Université, CRCI2NA, F-49 000, CHU Angers, France.
Blood Adv. 2025 Feb 25;9(4):797-807. doi: 10.1182/bloodadvances.2024014368.
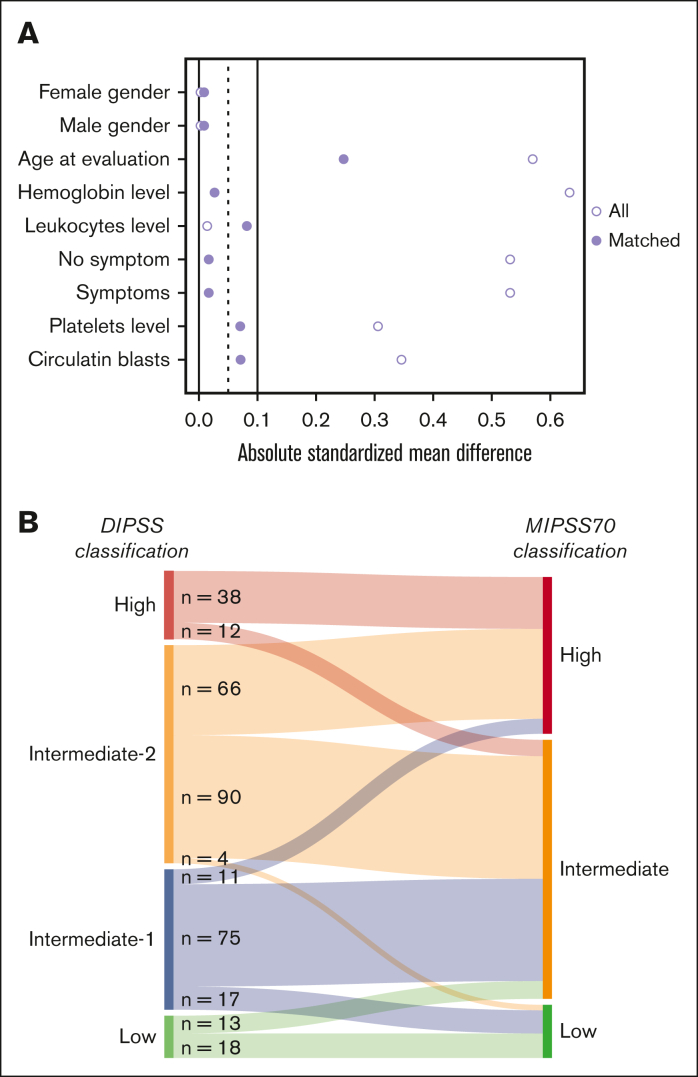
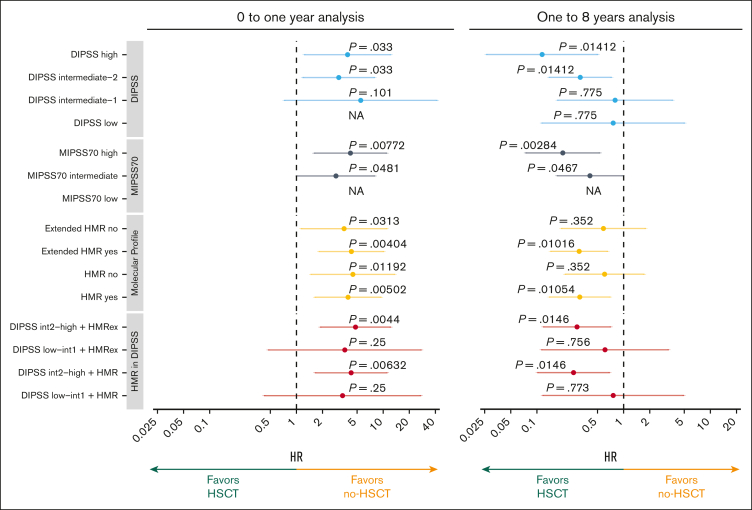
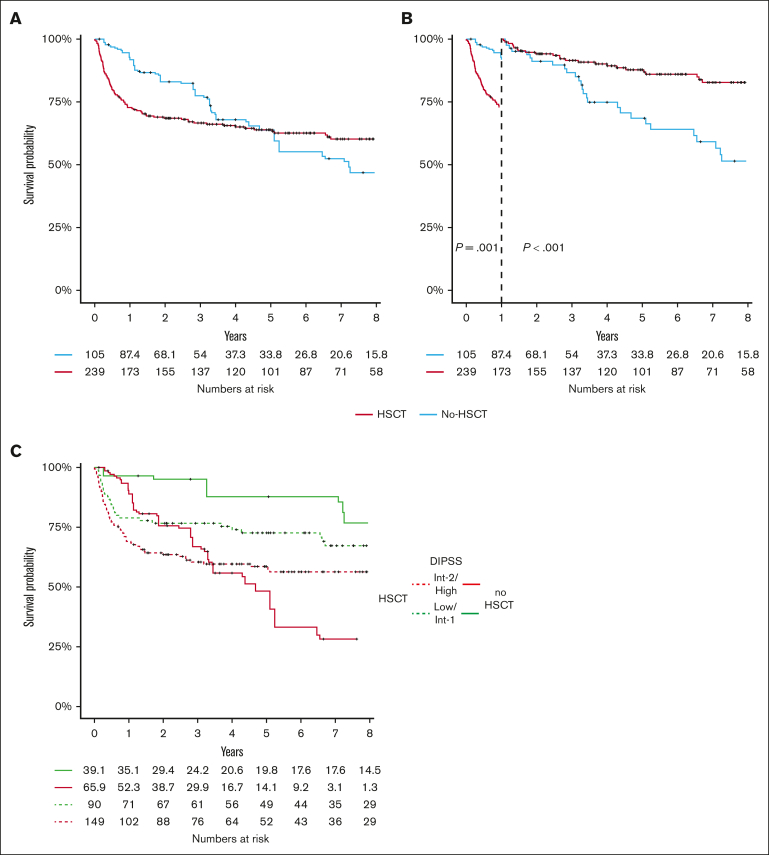
The aim of our study was to analyze the potential survival benefit associated with hematopoietic stem cell transplantation (HSCT) according to clinicobiological scores, which incorporate mutation-enhanced international prognostic score system (MIPSS) to facilitate decision-making in this context. One transplant (n = 241) and 1 nontransplant cohort (n = 239) were used to test the hypothesis that patients with primary myelofibrosis with higher risk molecular score benefit from HSCT. A weighted propensity score was applied to balance confounding factors with the transplanted cohort as reference. Weighted Cox proportional hazard models and logistic regression analyses were performed. Overall, 105 patients who did not receive transplant could be matched to the 239 patients who did receive transplants. HSCT was associated with a higher 6-year overall survival rate in intermediate-2 (60.1% vs 41.5%) and high-risk DIPSS patients (44.4% vs 6.55%), high-risk MIPSS70 (46.5% vs 23.9%), high-risk (73.2% vs 39.7%) or very high-risk MIPSS70+V2 (51.8% vs 24%). Patients with intermediate MIPSS70 scores have an advantage of survival with HSCT only when their myelofibrosis transplant scoring system (MTSS) were low or intermediate. Patients who received transplant had an increased mortality risk the first year, but a significant benefit with HSCT after the 1-year landmark was observed in higher risk patients. This study confirms that, similar to DIPSS, MIPSS70 and MIPSS70+V2 risk score in addition to MTSS can be used to determine which patients with primary myelofibrosis have survival benefit from HSCT over non-HSCT strategies.
我们研究的目的是根据临床生物学评分分析造血干细胞移植(HSCT)相关的潜在生存获益,该评分纳入了突变增强国际预后评分系统(MIPSS),以促进在此背景下的决策制定。一个移植队列(n = 241)和一个非移植队列(n = 239)被用于检验原发性骨髓纤维化分子风险评分较高的患者从HSCT中获益的假设。应用加权倾向评分以移植队列作为对照来平衡混杂因素。进行了加权Cox比例风险模型和逻辑回归分析。总体而言,105例未接受移植的患者可与239例接受移植的患者匹配。在中危-2(60.1%对41.5%)和高危DIPSS患者(44.4%对6.55%)、高危MIPSS70(46.5%对23.9%)、高危(73.2%对39.7%)或极高危MIPSS70+V2(51.8%对24%)患者中,HSCT与更高的6年总生存率相关。MIPSS70评分为中危的患者仅在其骨髓纤维化移植评分系统(MTSS)为低或中危时,接受HSCT有生存优势。接受移植的患者在第一年有更高的死亡风险,但在1年界标之后,观察到高危患者接受HSCT有显著获益。本研究证实,与DIPSS类似,除MTSS外,MIPSS70和MIPSS70+V2风险评分可用于确定哪些原发性骨髓纤维化患者接受HSCT比非HSCT策略有生存获益。