Department of Hematology and Hematopoietic Cell Transplantation.
Division of Biostatistics, Department of Information Sciences.
Blood Adv. 2019 Jan 8;3(1):83-95. doi: 10.1182/bloodadvances.2018026658.
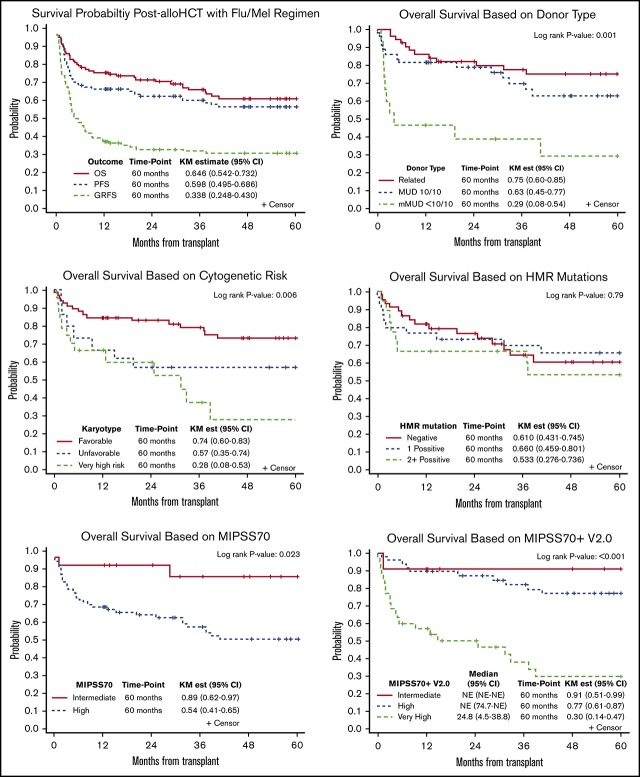
Although allogeneic hematopoietic cell transplantation (allo-HCT) is the only curative treatment for myelofibrosis (MF), data are limited on how molecular markers predict transplantation outcomes. We retrospectively evaluated transplantation outcomes of 110 consecutive MF patients who underwent allo-HCT with a fludarabine/melphalan (Flu/Mel) conditioning regimen at our center and assessed the impact of molecular markers on outcomes based on a 72-gene next-generation sequencing panel and Mutation-Enhanced International Prognostic Scoring System 70+ v2.0 (MIPSS70+ v2.0). With a median follow-up of 63.7 months, the 5-year overall survival (OS) rate was 65% and the nonrelapse mortality (NRM) rate was 17%. In mutational analysis, JAK2 V617F and ASXL1 mutations were the most common. By univariable analysis, higher Dynamic International Prognostic Scoring System scores, unrelated donor type, and very-high-risk cytogenetics were significantly associated with lower OS. Only CBL mutations were significantly associated with lower OS (hazard ratio [HR], 2.64; = .032) and increased NRM (HR, 3.68; = .004) after allo-HCT, but CALR, ASXL1, and IDH mutations did not have an impact on transplantation outcomes. Patient classification per MIPSS70 showed worse OS for high-risk (HR, 0.49; = .039) compared with intermediate-risk patients. Classification per MIPSS70+ v2.0 demonstrated better OS when intermediate-risk patients were compared with high-risk patients (HR, 0.291) and much lower OS when very-high-risk patients were compared with high-risk patients (HR, 5.05; ≤ .001). In summary, we present one of the largest single-center experiences of Flu/Mel-based allo-HCT, demonstrating that revised cytogenetic changes and MIPSS70+ v2.0 score predict transplantation outcomes, and thus can better inform physicians and patients in making decisions about allo-HCT.
虽然异基因造血细胞移植(allo-HCT)是骨髓纤维化(MF)的唯一治愈性治疗方法,但关于分子标志物如何预测移植结果的数据有限。我们回顾性评估了在我们中心接受氟达拉滨/美法仑(Flu/Mel)预处理方案的 110 例连续 MF 患者的移植结果,并根据 72 基因下一代测序面板和突变增强国际预后评分系统 70+ v2.0(MIPSS70+ v2.0)评估了分子标志物对结果的影响。中位随访 63.7 个月,5 年总生存率(OS)为 65%,非复发死亡率(NRM)为 17%。在突变分析中,JAK2 V617F 和 ASXL1 突变最为常见。单变量分析显示,较高的动态国际预后评分系统评分、无关供体类型和极高风险细胞遗传学与较低的 OS 显著相关。只有 CBL 突变与 allo-HCT 后较低的 OS(危险比[HR],2.64;P =.032)和增加的 NRM(HR,3.68;P =.004)显著相关,而 CALR、ASXL1 和 IDH 突变对移植结果没有影响。根据 MIPSS70 进行患者分类,高危患者的 OS 较差(HR,0.49;P =.039),与中危患者相比。根据 MIPSS70+ v2.0 进行分类时,与高危患者相比,中危患者的 OS 更好(HR,0.291),与高危患者相比,极高危患者的 OS 低得多(HR,5.05;P ≤.001)。总之,我们提供了基于 Flu/Mel 的 allo-HCT 的最大单中心经验之一,表明修订后的细胞遗传学变化和 MIPSS70+ v2.0 评分可预测移植结果,从而可以更好地为医生和患者提供关于 allo-HCT 的决策依据。