Department of Critical Care Medicine, Manipal Hospital Dhakuria, P-4 & 5, CIT Scheme, LXXII, Block-A, Gariahat Road, Kolkata, 700029, India.
Medanta Institute of Critical Care and Anesthesiology, Medanta-The Medicity, Gurugram, Haryana, India.
Crit Care. 2024 Nov 19;28(1):375. doi: 10.1186/s13054-024-05176-8.
Sepsis is a global health problem with high morbidity and mortality. Low- and middle-income countries have a higher incidence and poorer outcome with sepsis. Large epidemiological studies in sepsis using Sepsis-3 criteria, addressing the process of care and deriving predictors of mortality are scarce in India.
A multicentre, prospective sepsis registry was conducted using Sepsis 3 criteria of suspected or confirmed infection and SOFA score of 2 or more in 19 ICUs in India over a period of one year (August 2022-July 2023). All adult patients admitted to the Intensive Care Unit who fulfilled the Sepsis 3 criteria for sepsis and septic shock were included. Patient infected with Covid 19 were excluded. Patients demographics, severity, admission details, initial resuscitation, laboratory and microbiological data and clinical outcome were recorded. Performance improvement programs as recommended by the Surviving Sepsis guideline were noted from the participating centers. Patients were followed till discharge or death while in hospital.
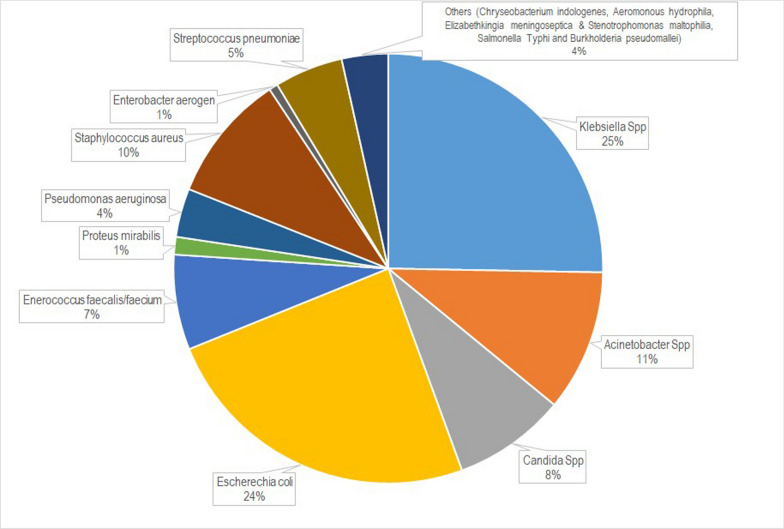
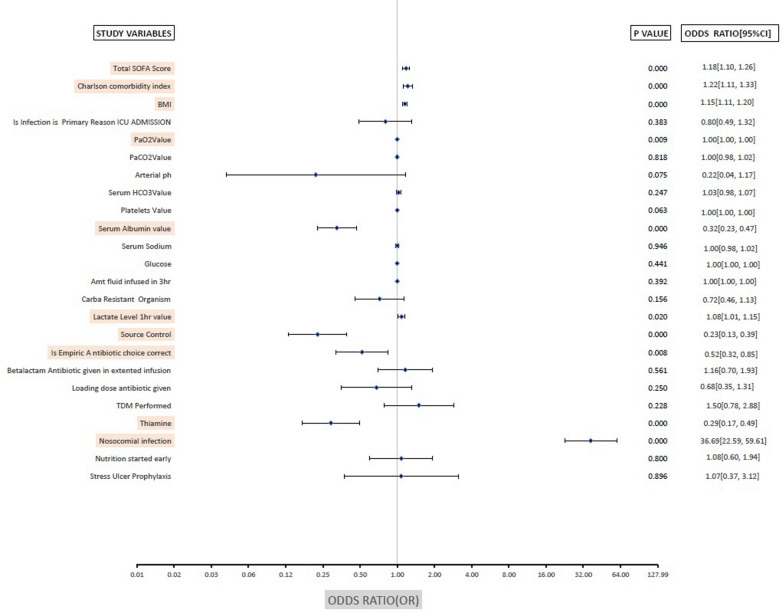
Registry Data of 1172 patients with sepsis (including 500 patients with septic shock) were analysed. The average age of the study cohort was 65 years, and 61% were male. The average APACHE II and SOFA score was 21 and 6.7 respectively. The majority of patients had community-acquired infections, and lung infections were the most common source. Of all culture positive results, 65% were gram negative organism. Carbapenem-resistance was identified in 50% of the gram negative blood culture isolates. The predominant gram negative organisms were Klebsiella spp (25%), Escherechia coli (24%) and Acinetobacter Spp (11%). Tropical infections (Dengue, Malaria, Typhus) constituted minority (n = 32, 2.2%) of sepsis patients. The observed hospital mortality for the entire cohort (n = 1172) was 36.3%, for those without shock (n = 672) it was 25.6% and for those with shock (n = 500) it was 50.8%. The average length of ICU and hospital stay for the study cohort was 8.64 and 11.9 respectively. In multivariate analysis adequate source control, correct choice of empiric antibiotic and the use of intravenous thiamine were protective.
The general demographics of the sepsis population in the Indian Sepsis Registry is comparable to Western population. The mortality of sepsis cohort was higher (36.3%) but septic shock mortality (50.8%) was comparable to Western reports. Gram negative infection was the predominant cause of sepsis with a high incidence of carbapenem resistance. Eschericia coli, Klebsiella Spp and Acinetobacter Spp were the predominant causative organism. Tropical infection constituted a minority of sepsis population with low hospital mortality. The SOFA score on admission was a comparatively better predictor of poor outcome. Sepsis secondary to nosocomial infections had the worst outcomes, while source control, correct empirical antibiotic selection, and intravenous thiamine were protective. CTRI Registration CTRI:2022/07/044516.
脓毒症是一个全球性的健康问题,发病率和死亡率都很高。中低收入国家的脓毒症发病率更高,预后更差。印度使用 Sepsis-3 标准进行的大型脓毒症流行病学研究,涉及护理过程,并得出死亡率预测因素,相对较少。
在印度的 19 个 ICU 中,使用 Sepsis-3 标准(疑似或确诊感染,SOFA 评分≥2)进行了一项多中心、前瞻性脓毒症登记研究,时间为一年(2022 年 8 月至 2023 年 7 月)。纳入所有符合 Sepsis-3 标准的脓毒症和脓毒性休克成人患者。感染新冠病毒的患者被排除在外。记录患者的人口统计学、严重程度、入院细节、初始复苏、实验室和微生物学数据以及临床结局。从参与中心注意到了《拯救脓毒症运动》指南推荐的绩效改进计划。患者在住院期间或出院时进行随访。
对 1172 例脓毒症患者(包括 500 例脓毒性休克患者)的登记数据进行了分析。研究队列的平均年龄为 65 岁,61%为男性。平均 APACHE II 和 SOFA 评分为 21 和 6.7。大多数患者有社区获得性感染,肺部感染是最常见的感染源。所有培养阳性结果中,65%为革兰氏阴性菌。革兰氏阴性菌血培养分离株中 50%为碳青霉烯耐药菌。主要的革兰氏阴性菌为肺炎克雷伯菌(25%)、大肠杆菌(24%)和不动杆菌(11%)。热带感染(登革热、疟疾、斑疹伤寒)在脓毒症患者中占少数(n=32,2.2%)。整个队列(n=1172)的住院死亡率为 36.3%,无休克者(n=672)为 25.6%,休克者(n=500)为 50.8%。研究队列的 ICU 和住院平均时间分别为 8.64 天和 11.9 天。多变量分析显示,充分的源头控制、正确选择经验性抗生素和使用静脉注射硫胺素具有保护作用。
印度脓毒症登记研究中脓毒症患者的一般人口统计学特征与西方人群相似。脓毒症患者的死亡率较高(36.3%),但脓毒性休克死亡率(50.8%)与西方报告相当。革兰氏阴性感染是脓毒症的主要原因,碳青霉烯耐药率较高。大肠杆菌、肺炎克雷伯菌和鲍曼不动杆菌是主要的致病微生物。热带感染在脓毒症患者中占少数,住院死亡率较低。入院时的 SOFA 评分是较差预后的一个较好的预测指标。医院获得性感染引起的脓毒症预后最差,而源头控制、正确的经验性抗生素选择和静脉注射硫胺素具有保护作用。CTRI 注册号:CTRI/2022/07/044516。