Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University College of Medicine, Sanggye Paik Hospital, Seoul, Republic of Korea.
Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, Korea.
Crit Care. 2024 Nov 25;28(1):385. doi: 10.1186/s13054-024-05151-3.
The distinction between culture-positive sepsis and culture-negative sepsis regarding clinical characteristics and outcomes remains contentious. We aimed to elucidate these differences using large-scale nationwide data.
This prospective cohort study analyzed data from the Korean Sepsis Alliance registry, comprising 21 intensive care units (ICUs) across 20 hospitals from September 2019 to December 2021. Patients meeting the Sepsis-3 criteria were included.
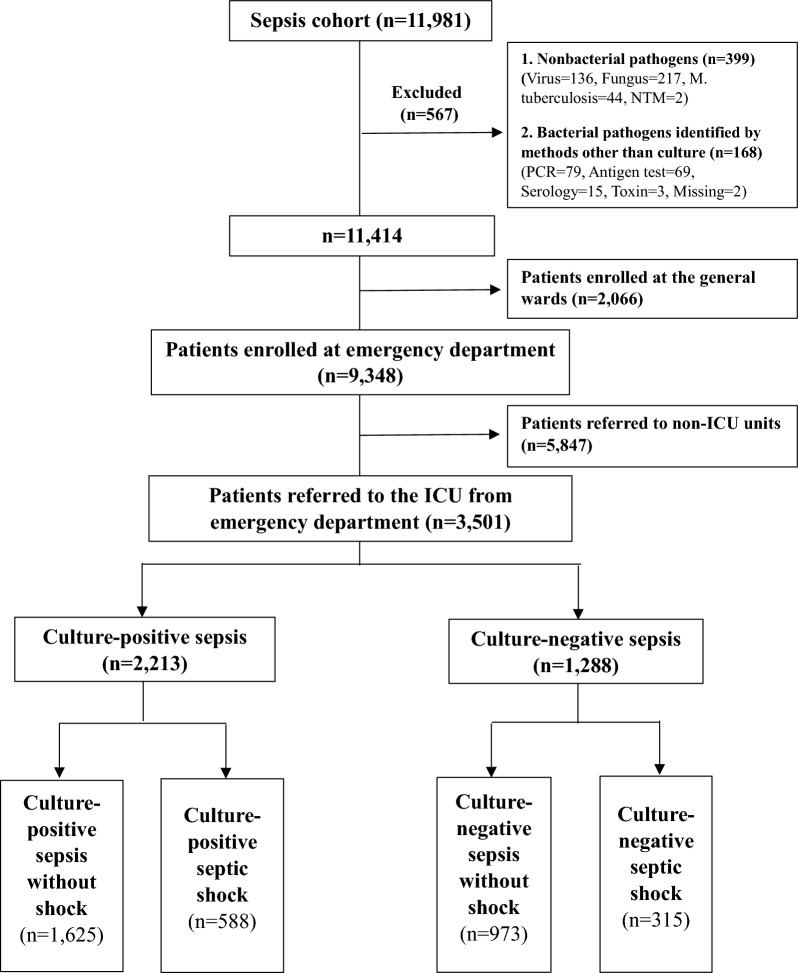
Among 11,981 sepsis patients, 3501 were analyzed, all of whom were referred to the ICU through the emergency department (mean age: 72 ± 13 years; 1976 [56%] males). Of these, 2213 (63%) were culture-positive sepsis and 1288 (37%) were culture-negative sepsis. Compared to the culture-positive sepsis group, the culture-negative sepsis group exhibited less severe illness, with lower Sequential Organ Failure Assessment scores and less deteriorated vital signs. While pulmonary-origin sepsis was common in both groups, culture-negative patients primarily presented with pulmonary infections and had a higher incidence of respiratory failure. In comparison to the culture-positive sepsis group, blood cultures and the administration of empirical antibiotics were performed less promptly in the culture-negative sepsis group. Patients with culture-negative sepsis also showed lower compliance with fluid resuscitation (98.4% vs. 96.9%, p = 0.038; culture-positive sepsis vs. culture-negative sepsis) and received vasopressors earlier (31.1% vs. 35.9%, p = 0.012). In-hospital mortality did not differ significantly between the two groups (31.6% vs. 34.9%, p = 0.073); however, in patients with septic shock, culture-negative sepsis had higher mortality rates (37.6% vs. 45.1%, p = 0.029). The apparent appropriateness of empirical antibiotics in the culture-negative septic shock was higher than that of the culture-positive septic shock (85.2% vs. 96.8%, p < 0.001). Culture-negativity independently predicted poor prognosis in septic shock patients (OR: 1.462, 95% CI [1.060-2.017], p = 0.021).
In patients with septic shock, culture-negativity was associated with increased mortality, despite the paradoxically higher appropriateness of empirical antibiotics than culture-positive patients. These contradictory findings suggest that the current criteria for determining the appropriateness of empirical antibiotic therapy may not be valid for culture-negative sepsis.
关于临床特征和结局,阳性菌血症性脓毒症和阴性菌血症性脓毒症之间的区别仍存在争议。我们旨在使用大规模全国性数据阐明这些差异。
本前瞻性队列研究分析了来自韩国脓毒症联盟登记处的数据,该登记处包括 2019 年 9 月至 2021 年 12 月期间 20 家医院的 21 个重症监护病房(ICU)。符合 Sepsis-3 标准的患者被纳入研究。
在 11981 例脓毒症患者中,分析了 3501 例患者,所有患者均通过急诊部门被转至 ICU(平均年龄:72±13 岁;1976 例[56%]为男性)。其中,2213 例(63%)为阳性菌血症性脓毒症,1288 例(37%)为阴性菌血症性脓毒症。与阳性菌血症性脓毒症组相比,阴性菌血症性脓毒症组的病情较轻,序贯器官衰竭评估评分较低,生命体征恶化程度较轻。两组中肺部来源的脓毒症均很常见,但阴性菌血症患者主要表现为肺部感染,呼吸衰竭的发生率较高。与阳性菌血症性脓毒症组相比,阴性菌血症性脓毒症组血培养和经验性抗生素治疗的实施时间较晚。阴性菌血症性脓毒症患者的液体复苏依从性也较低(98.4%比 96.9%,p=0.038;阳性菌血症性脓毒症组比阴性菌血症性脓毒症组),且更早使用升压药(31.1%比 35.9%,p=0.012)。两组患者的院内死亡率无显著差异(31.6%比 34.9%,p=0.073);然而,在脓毒性休克患者中,阴性菌血症性脓毒症的死亡率更高(37.6%比 45.1%,p=0.029)。阴性菌血症性脓毒性休克患者经验性抗生素治疗的明显适宜性高于阳性菌血症性脓毒性休克(85.2%比 96.8%,p<0.001)。在脓毒性休克患者中,阴性菌血症与不良预后独立相关(OR:1.462,95%CI[1.060-2.017],p=0.021)。
在脓毒性休克患者中,尽管经验性抗生素治疗的适宜性似乎高于阳性菌血症患者,但阴性菌血症与死亡率增加相关。这些矛盾的发现表明,目前用于确定经验性抗生素治疗适宜性的标准可能不适用于阴性菌血症性脓毒症。