White Brooke E, Hodo Carolyn L, Hamer Sarah A, Saunders Ashley B, Laucella Susana A, Hall Daniel B, Tarleton Rick L
Center for Tropical and Emerging Global Disease, University of Georgia, Athens, Georgia, USA.
Michale E. Keeling Center for Comparative Medicine and Research, The University of Texas MD Anderson Cancer Center, Bastrop, Texas, USA.
bioRxiv. 2024 Nov 5:2024.06.10.598182. doi: 10.1101/2024.06.10.598182.
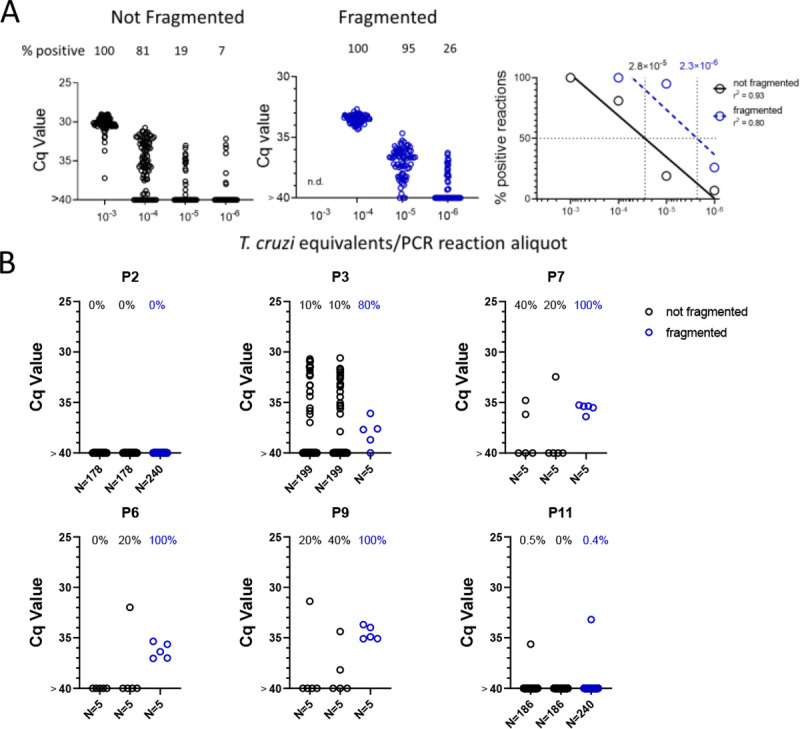
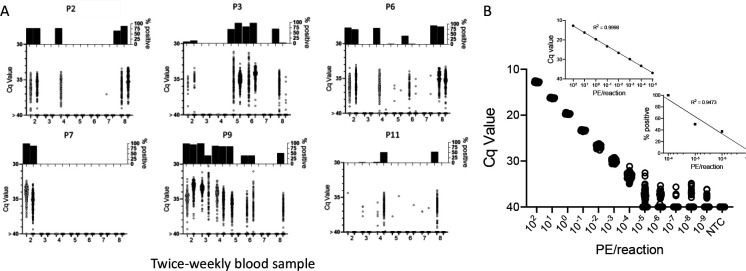
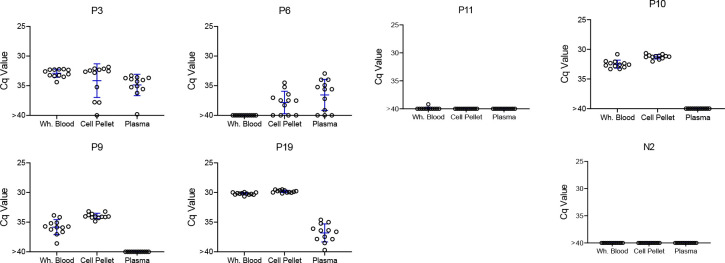
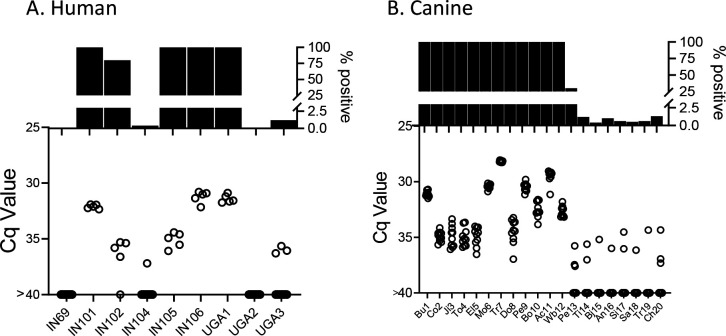
Infection with the protozoan parasite is generally well-controlled by host immune responses, but appears to be rarely eliminated. The resulting persistent, low-level infection results in cumulative tissue damage with the greatest impact generally in the heart in the form of chagasic cardiomyopathy. The relative success in immune control of infection usually averts acute phase death but has the negative consequence that the low-level presence of in hosts is challenging to detect unequivocally. Thus, it is difficult to identify those who are actively infected and, as well, problematic to gauge the impact of treatment, particularly in the evaluation of the relative efficacy of new drugs. In this study we employ DNA fragmentation and high numbers of replicate PCR reaction ('deep-sampling') to extend the quantitative range of detecting in blood by at least 3 orders of magnitude relative to current protocols. When combined with sampling blood at multiple time points, deep sampling of fragmented DNA allowed for detection of in all infected hosts in multiple host species. In addition, we provide evidence for a number of characteristics not previously rigorously quantified in the population of hosts with naturally acquired infection, including, a > 6-log variation between chronically infected individuals in the stable parasite levels, a continuing decline in parasite load during the second and third years of infection in some hosts, and the potential for parasite load to change dramatically when health conditions change. Although requiring strict adherence to contamination-prevention protocols and significant resources, deep-sampling PCR provides an important new tool for assessing new therapies and for addressing long-standing questions in infection and Chagas disease.
原生动物寄生虫感染通常能被宿主免疫反应很好地控制,但似乎很少能被清除。由此产生的持续性低水平感染会导致累积性组织损伤,其中对心脏的影响最大,表现为恰加斯心肌病。在免疫控制寄生虫感染方面取得的相对成功通常能避免急性期死亡,但有一个负面后果,即宿主中低水平的寄生虫存在难以明确检测到。因此,很难确定哪些人是活跃感染者,而且评估治疗效果也存在问题,尤其是在评估新药的相对疗效时。在本研究中,我们采用DNA片段化和大量重复PCR反应(“深度采样”),相对于当前方案,将血液中检测寄生虫的定量范围至少扩大3个数量级。当与在多个时间点采集血液相结合时,对片段化DNA进行深度采样能够在多种宿主物种的所有感染宿主中检测到寄生虫。此外,我们提供了一些证据,证明在自然感染寄生虫的宿主群体中,有一些特征以前没有得到严格量化,包括慢性感染个体之间稳定寄生虫水平存在>6个对数的差异,一些宿主在感染的第二和第三年寄生虫载量持续下降,以及健康状况改变时寄生虫载量可能会发生巨大变化。尽管需要严格遵守污染预防方案并投入大量资源,但深度采样PCR为评估新疗法以及解决寄生虫感染和恰加斯病方面长期存在的问题提供了一种重要的新工具。