Padavia Faheemah, Treluyer Jean-Marc, Cambonie Gilles, Flamant Cyril, Rideau Aline, Tauzin Manon, Patkai Juliana, Gascoin Géraldine, Lumia Mirka, Aikio Outi, Foissac Frantz, Urien Saïk, Benaboud Sihem, Lui Gabrielle, Froelicher Bournaud Léo, Zheng Yi, Kemper Ruth, Tortigue Marine, Baruteau Alban-Elouen, Kallio Jaana, Hallman Mikko, Diallo Alpha, Levoyer Léa, Roze Jean-Christophe, Bouazza Naïm
URP7323 Université Paris Cité, Pharmacologie et évaluations des thérapeutiques chez l'enfant et la femme enceinte, Hôpital Tarnier, 89 rue d'Assas, 75006, Paris, France.
Unité de Recherche Clinique, Université Paris Cité Necker/Cochin, Hôpital Tarnier, Paris, France.
Clin Pharmacokinet. 2024 Dec;63(12):1689-1700. doi: 10.1007/s40262-024-01439-3. Epub 2024 Nov 22.
Our aim was to describe the pharmacokinetics of paracetamol and its metabolites in extreme preterm neonates in the context of patent ductus arteriosus treatment. Factors associated with inter-individual variability and metabolic pathways were studied. The association between drug exposure and clinical outcomes were investigated.
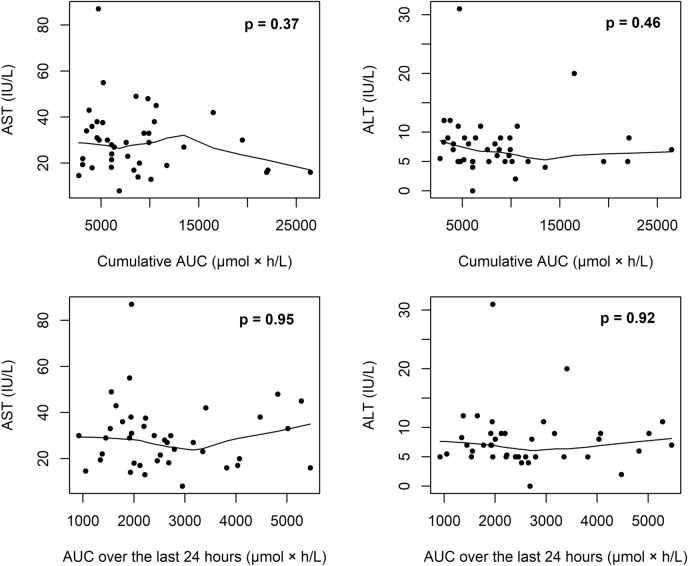
Preterm neonates of 23-26 weeks' gestational age received paracetamol within 12 h after birth. Plasma concentrations of paracetamol and its metabolites were measured throughout 5 days of treatment. Clinical success was defined as ductus closure on two consecutive days or at day 7. Aspartate aminotransferase and alanine aminotransferase levels were used as surrogates for liver damage.
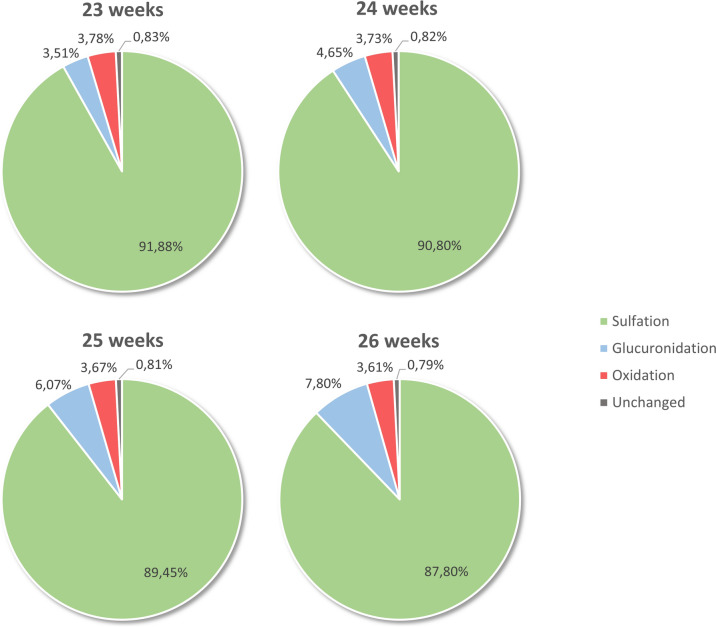
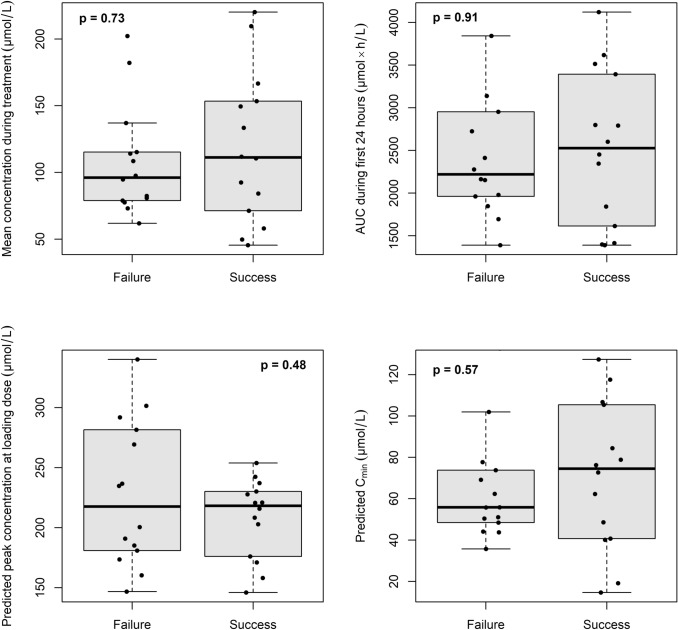
Data from 30 preterm neonates were available for pharmacokinetic analysis. Paracetamol pharmacokinetics were described using a two-compartment model with significant positive effects of weight on clearance and of birth length on peripheral compartment volume. Paracetamol was mainly metabolised into sulphate (89%) then glucuronide (6%), and the oxidative metabolic pathway was reduced (4%). The glucuronidation pathway increased with gestational age, whereas the sulfation pathway decreased. No difference was observed in drug exposure between successful and unsuccessful patients. No increase in aspartate aminotransferase and alanine aminotransferase levels were observed during treatment, and no association was found with either paracetamol or oxidative metabolite exposures.
The relative proportions of the metabolic pathways were characterised with gestational age. In the range of observed drug exposures, no association was found with clinical response or liver biomarkers. These findings may suggest that paracetamol concentrations were within the range that already guarantee a maximum effect on ductus closure.
我们的目的是描述在动脉导管未闭治疗背景下,对极早产儿扑热息痛及其代谢物的药代动力学。研究了个体间变异性和代谢途径相关因素。调查了药物暴露与临床结局之间的关联。
孕龄23 - 26周的早产儿在出生后12小时内接受扑热息痛治疗。在整个5天的治疗过程中测量扑热息痛及其代谢物的血浆浓度。临床成功定义为连续两天或第7天动脉导管关闭。使用天冬氨酸转氨酶和丙氨酸转氨酶水平作为肝损伤的替代指标。
30例早产儿的数据可用于药代动力学分析。扑热息痛药代动力学采用二室模型描述,体重对清除率有显著正向影响,出生身长对外周室容积有显著正向影响。扑热息痛主要代谢为硫酸盐(89%),然后是葡萄糖醛酸苷(6%),氧化代谢途径减少(4%)。葡萄糖醛酸化途径随孕周增加,而硫酸化途径减少。成功和未成功患者之间在药物暴露方面未观察到差异。治疗期间未观察到天冬氨酸转氨酶和丙氨酸转氨酶水平升高,且未发现与扑热息痛或氧化代谢物暴露有相关性。
代谢途径的相对比例与孕周有关。在观察到的药物暴露范围内,未发现与临床反应或肝脏生物标志物有相关性。这些发现可能表明扑热息痛浓度在已能保证对动脉导管关闭产生最大效果的范围内。