Department of Medicine (Neurology & Rheumatology), Shinshu University School of Medicine, Matsumoto, Japan.
Center for Medical Genetics, Shinshu University Hospital, Matsumoto, Japan.
Mol Genet Genomic Med. 2024 Nov;12(11):e70044. doi: 10.1002/mgg3.70044.
Heterozygous variants of sequestosome-1 gene (SQSTM1) have been reported in patients with various neurological disorders, whereas biallelic pathogenic variants of SQSTM1 can cause child-onset and multisystem neurodegeneration, including cerebellar ataxia, dystonia, and vertical gaze palsy (NADGP). Here, we describe two cases of NADGP in a Japanese family.
We performed clinical and genetic laboratory evaluations of the two patients and their healthy parents.
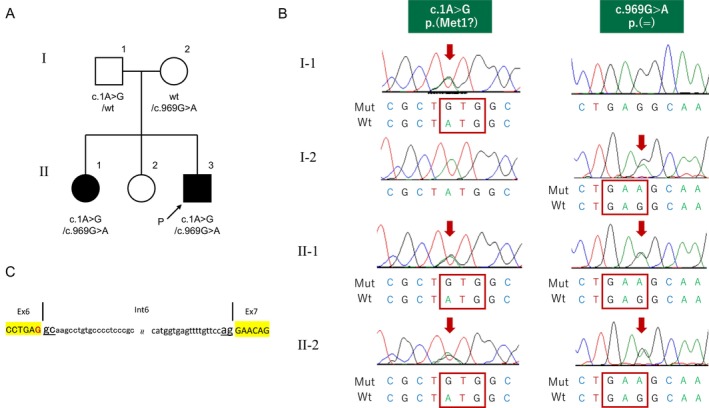
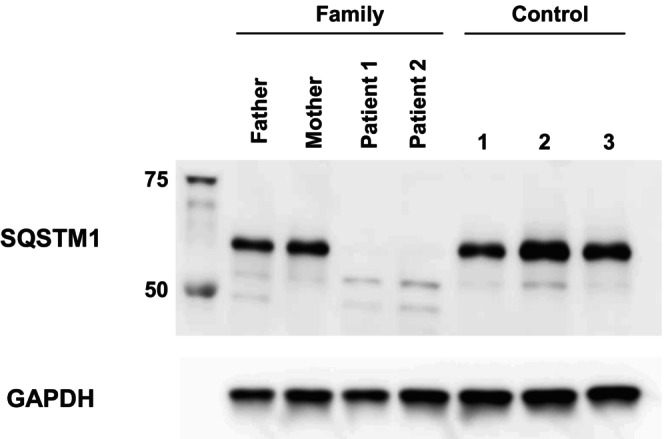
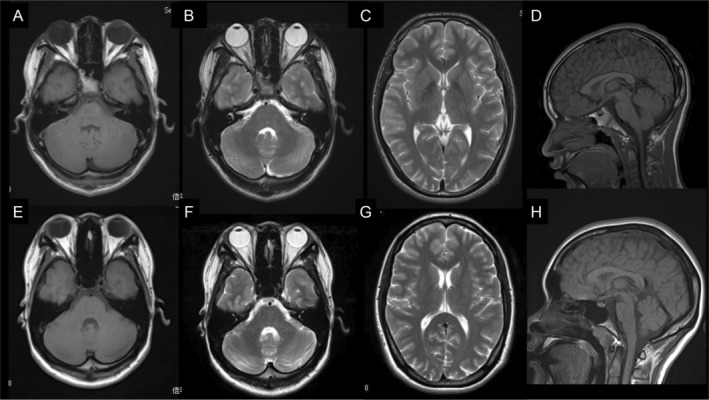
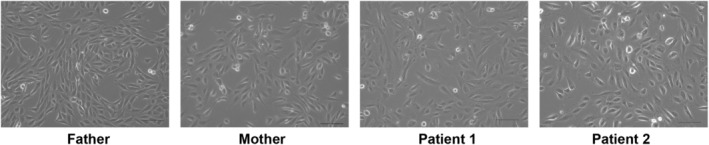
By whole-exome sequencing, we identified compound heterozygous variants in SQSTM1(NM_003900.5): c.1A>G p.(Met1?) in the initial codon, and c.969G>A, located at the 3' end of exon 6, which is novel and seemingly a synonymous but is actually a truncating variant causing aberrant splicing. An SQSTM1 protein expression assay using urine-derived cells (UDCs) demonstrated that both variants (c.1A>G and c.969G>A) were unable to induce normal splicing of premessenger RNA. Cerebellar ataxia is a characteristic manifestation of this disorder; however, brain magnetic resonance imaging studies have not shown significant cerebellar atrophy. Our patients experienced chorea during adolescence.
Only a few reports have highlighted the presence of chorea; however, our findings suggest that NADGP should be considered as a differential diagnosis of hereditary chorea. This study also demonstrates the utility of UDCs, obtained using noninvasive approaches, in functionally analyzing genetic diseases.
已在各种神经疾病患者中报道了 sequestosome-1 基因 (SQSTM1) 的杂合变体,而 SQSTM1 的双等位致病性变体可导致儿童发病和多系统神经退行性变,包括小脑性共济失调、肌张力障碍和垂直性眼球运动麻痹 (NADGP)。在此,我们描述了一个日本家族中的两例 NADGP。
我们对这两名患者及其健康父母进行了临床和遗传实验室评估。
通过全外显子组测序,我们在 SQSTM1 (NM_003900.5) 中发现了复合杂合变体:起始密码子处的 c.1A>G p.(Met1?),以及位于外显子 6 末端的 c.969G>A,这是一个新的、看似同义但实际上是导致异常剪接的截断变体。使用尿源性细胞 (UDC) 进行的 SQSTM1 蛋白表达测定表明,这两个变体 (c.1A>G 和 c.969G>A) 均无法诱导前信使 RNA 的正常剪接。小脑性共济失调是该疾病的特征性表现;然而,脑部磁共振成像研究并未显示明显的小脑萎缩。我们的患者在青春期出现舞蹈症。
仅有少数报道强调了舞蹈症的存在;然而,我们的发现表明,NADGP 应被视为遗传性舞蹈症的鉴别诊断。本研究还表明,使用非侵入性方法获得的 UDC 可用于遗传疾病的功能分析。