Zaaroura Hiba, Tibi Afik, Avitan-Hersh Emily, Khamaysi Ziad
Department of Dermatology, Rambam Health Care Campus, 8th Ha'aliya Hashnia, 3109601, Haifa, Israel.
Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel.
Adv Ther. 2025 Jan;42(1):537-547. doi: 10.1007/s12325-024-03017-2. Epub 2024 Nov 26.
Infantile hemangioma (IH) is a common benign tumor in infants. While most cases exhibit a self-limiting nature, some require medical treatment to avoid complications. Propranolol is the first-line therapy for IH, it has a high success rate, and is safe to use. Unfortunately, some patients might experience rebound growth after propranolol discontinuation. Currently, it is unclear which factors predict this phenomenon. This study aimed to identify factors affecting the rebound growth of IH after propranolol cessation. We also aimed to identify predictors for an excellent response to oral propranolol.
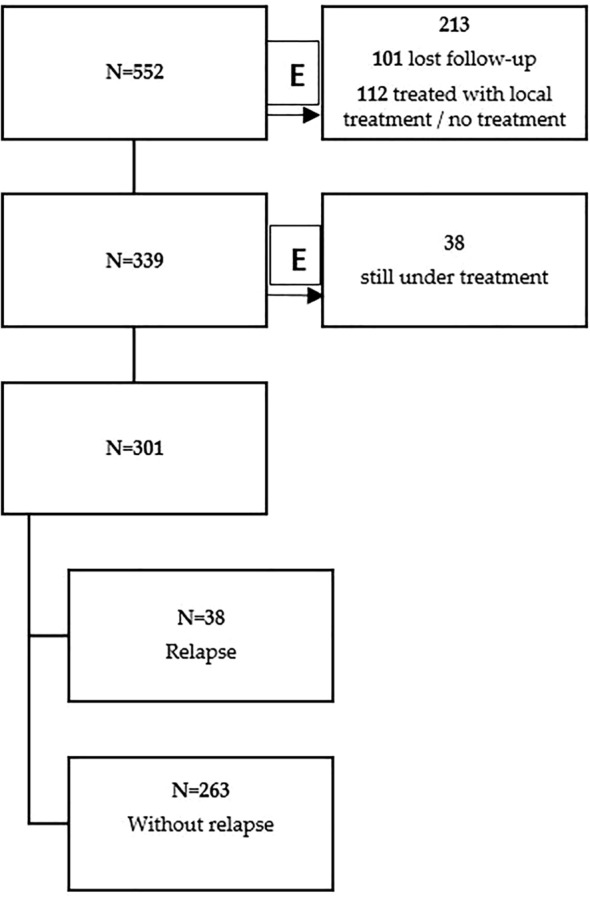
We performed a retrospective cohort study using clinical data from all patients referred to our clinic with IH and placed on systemic oral propranolol between January 2009 to December 2023 in the dermatology outpatient clinic of Rambam Healthcare Campus.
Out of a total of 552 patients with IH, 301 received oral propranolol for at least 6 months. A relapse phenomenon was observed in 38 (12.6%) patients. We found a significant association between limb involvement and the least likelihood of hemangioma rebound (p < 0.001). An excellent response to oral propranolol was observed in 57.8% of patients. Younger age at initiation of oral propranolol was associated with an excellent response (p = 0.015). Also, IHs located on the limbs (67) showed a higher rate of excellent response to oral propranolol compared to other anatomical sites (p = 0.02). Interestingly, patients who were treated with a dose of 2 mg/kg/day were associated with excellent response to treatment (p = 0.007).
IHs located on the limbs demonstrated less rebound growth and a better treatment response. When oral propranolol was initiated earlier or when the target dose was 2 mg/kg/day, there was a higher rate of excellent response to treatment.
婴儿血管瘤(IH)是婴儿常见的良性肿瘤。虽然大多数病例具有自限性,但有些需要医学治疗以避免并发症。普萘洛尔是IH的一线治疗药物,成功率高且使用安全。不幸的是,一些患者在停用普萘洛尔后可能会出现瘤体反弹生长。目前,尚不清楚哪些因素可预测这一现象。本研究旨在确定影响普萘洛尔停药后IH反弹生长的因素。我们还旨在确定口服普萘洛尔治疗效果极佳的预测因素。
我们进行了一项回顾性队列研究,使用2009年1月至2023年12月在兰巴姆医疗中心皮肤科门诊就诊并接受系统性口服普萘洛尔治疗的所有IH患者的临床数据。
在总共552例IH患者中,301例接受口服普萘洛尔治疗至少6个月。38例(12.6%)患者出现复发现象。我们发现肢体受累与血管瘤反弹可能性最小之间存在显著关联(p < 0.001)。57.8%的患者口服普萘洛尔治疗效果极佳。口服普萘洛尔起始年龄较小与治疗效果极佳相关(p = 0.015)。此外,位于肢体的IH(67例)与其他解剖部位相比,对口服普萘洛尔治疗效果极佳的比例更高(p = 0.02)。有趣的是,接受2mg/kg/天剂量治疗的患者与治疗效果极佳相关(p = 0.007)。
位于肢体的IH显示出较少的反弹生长和更好的治疗反应。当更早开始口服普萘洛尔或目标剂量为2mg/kg/天时,治疗效果极佳的比例更高。