Department of Radiation Oncology, University Leipzig Medical Center, Stephanstraße 9a, 04103, Leipzig, Germany.
Comprehensive Cancer Center Central Germany (CCCG), 04103, Leipzig, Germany.
Acta Neuropathol Commun. 2024 Nov 26;12(1):180. doi: 10.1186/s40478-024-01889-7.
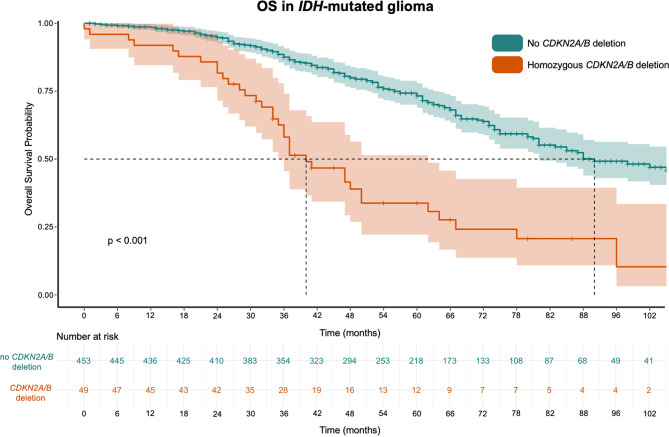
CDKN2A/B deletions are prognostically relevant in low- and high-grade gliomas. Data on this is derived from heterogeneous series, an accurate estimation of survival risk from homozygous CDKN2A/B deletion is missing. Besides genetic testing, p16-immunohistochemistry (IHC) as a less cost intensive means for indirect detection of CDKN2A/B alterations is possible but not validated in larger datasets. The present meta-analysis aimed to (1) reconstruct individual patient data (IPD) and estimate overall survival (OS) stratified by CDKN2A/B status from all literature and to (2) determine accuracy of p16 testing for CDKNA2/B detection from published studies. For survival analysis according to CDKN2A/B status 460 records were screened, four articles with 714 participants were included. In IDH-wildtype (IDH-wt) gliomas, 57.07% harbored the deletion compared to 9.76% in IDH-mutant (IDH-mut) gliomas. Median OS of patients with IDH-wt gliomas and homozygous CDKN2A/B deletion was 13.0 months compared to 18.0 months with non-deleted CDKN2A/B (p = 0.014, Log-Rank). With homozygous deletion of CDKN2A/B the risk of death was increased by 1.5 (95%-CI 1.1-2.1). Median OS in patients with IDH-mut gliomas without CDKN2A/B deletion was 92.0 months compared to 40.0 months with CDKN2A/B deletion (p < 0.001, Log-Rank). CDKN2A/B deletions were associated with a significantly shorter OS (HR = 3.2; 95%-CI 2.2-5.5). For p16 IHC analysis, 10 eligible studies with 1087 examined samples were included. The cut-off for retention differed between the studies. In 588/662 p16 retained cases CDKN2A/B deletions was not detected, implying a negative predictive value (NPV) of p16 staining of 88.8%. Conversely, 279/425 p16 absent cases showed a CDKN2A/B deletion resulting in a positive predictive value (PPV) of 65.6%. Sensitivity of p16 staining for CDKN2A/B detection was 79.0%, specificity 80.1%. Highest diagnostic accuracy of p16 IHC was reached with a cut-off of > 5% and within IDH-mut glioma.
CDKN2A/B 缺失与低级别和高级别神经胶质瘤的预后相关。这方面的数据来自于异质系列,缺乏对纯合性 CDKN2A/B 缺失的生存风险的准确估计。除了基因检测外,p16 免疫组化(IHC)作为一种间接检测 CDKN2A/B 改变的成本较低的方法是可能的,但在更大的数据集上尚未得到验证。本荟萃分析旨在:(1)从所有文献中重建个体患者数据(IPD)并估计按 CDKN2A/B 状态分层的总生存率(OS);(2)确定 p16 检测用于检测 CDKNA2/B 的准确性来自已发表的研究。为了根据 CDKN2A/B 状态进行生存分析,筛选了 460 条记录,纳入了 4 篇文章共 714 名参与者。在 IDH 野生型(IDH-wt)神经胶质瘤中,57.07%携带缺失,而 IDH 突变型(IDH-mut)神经胶质瘤中仅为 9.76%。IDH-wt 神经胶质瘤患者中携带纯合性 CDKN2A/B 缺失的中位 OS 为 13.0 个月,而非缺失 CDKN2A/B 的中位 OS 为 18.0 个月(p=0.014,对数秩)。携带纯合性 CDKN2A/B 缺失的患者死亡风险增加 1.5 倍(95%-CI 1.1-2.1)。IDH-mut 神经胶质瘤患者中无 CDKN2A/B 缺失的中位 OS 为 92.0 个月,而有 CDKN2A/B 缺失的中位 OS 为 40.0 个月(p<0.001,对数秩)。CDKN2A/B 缺失与显著缩短的 OS 相关(HR=3.2;95%-CI 2.2-5.5)。对于 p16 IHC 分析,纳入了 10 项研究共 1087 个检查样本。保留的截止值在研究之间存在差异。在 662 例 p16 保留病例中未检测到 CDKN2A/B 缺失,这意味着 p16 染色的阴性预测值(NPV)为 88.8%。相反,在 425 例 p16 缺失病例中,有 279 例显示 CDKN2A/B 缺失,这导致阳性预测值(PPV)为 65.6%。p16 染色检测 CDKN2A/B 的敏感性为 79.0%,特异性为 80.1%。在 IDH-mut 神经胶质瘤中,p16 IHC 的最高诊断准确性达到了>5%的截断值。