Ivanov Dmytro, Weber Lutz T, Levtchenko Elena, Vakulenko Liudmyla, Ivanova Mariia, Zavalna Iryna, Lagodych Yelizaveta, Boiko Ninel
Institute of Postgraduate Education, Bogomolets National Medical University, 01601 Kyiv, Ukraine.
German Society for Pediatric Nephrology, 10963 Berlin, Germany.
Biomedicines. 2024 Nov 13;12(11):2600. doi: 10.3390/biomedicines12112600.
Steroid-sensitive nephrotic syndrome (SSNS) and steroid-resistant nephrotic syndrome (SRNS) significantly affect children's quality of life. There are frequent relapses in SSNS and progression in SRNS. IPNA guidelines suggest that monoclonal antibodies like rituximab (RTX) are promising treatments.
This study aims to evaluate the long-term efficacy and safety of rituximab administration in children with SSNS, encompassing FRNS and SDNS, and SRNS over a two-year follow-up period, facilitating individualized management.
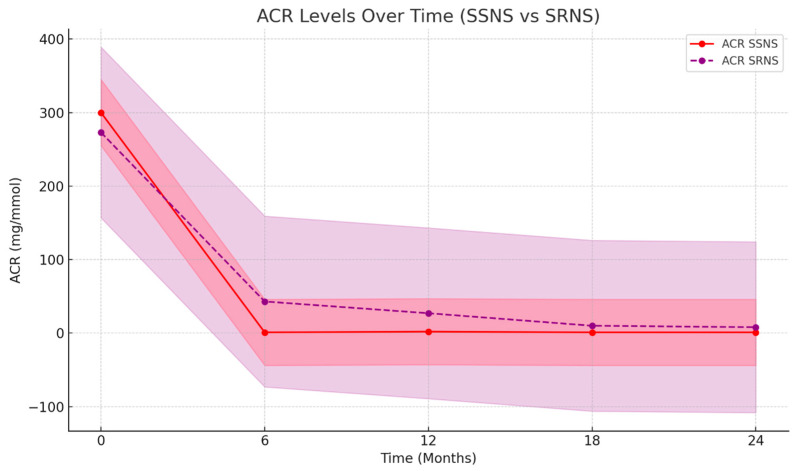
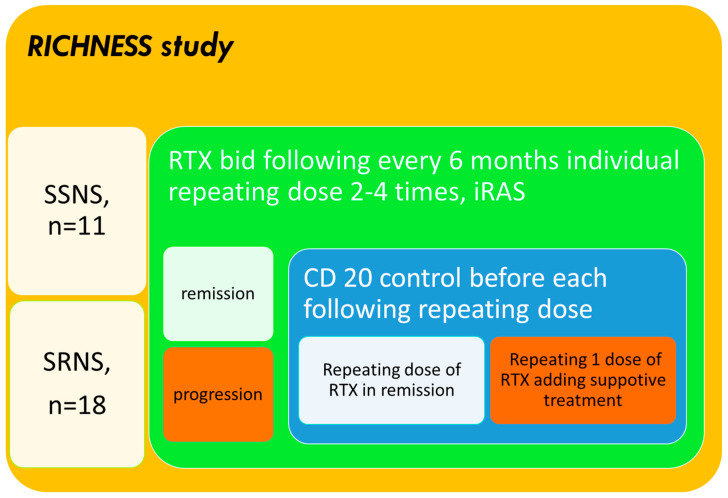
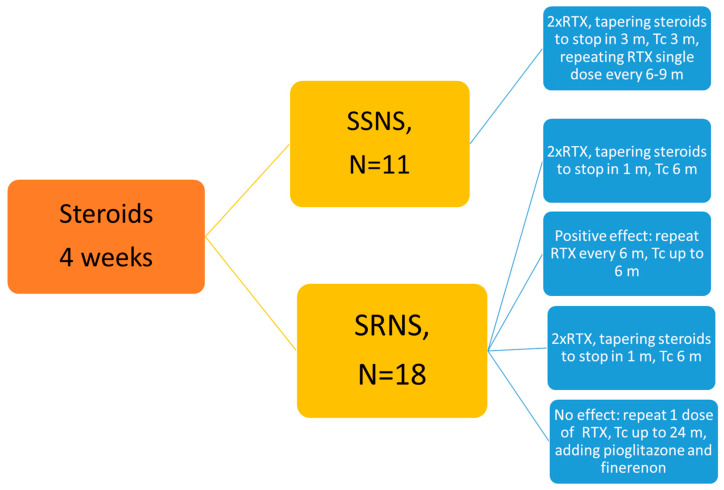
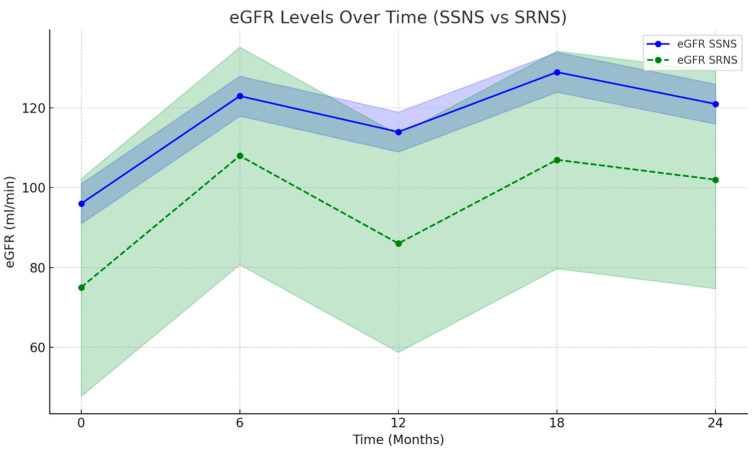
We conducted an open-label, multicenter, randomized, and patient-oriented study (RICHNESS), involving children aged 3-18 with SRNS (18) and SSNS (11) undergoing 2 years continuous RTX therapy. The primary outcome was complete/partial remission (CR/PR), as defined by IPNA/KDIGO guidelines, at 6, 12, 18, and 24 months on RTX; secondary outcomes included adverse events. Key endpoints included the estimated glomerular filtration rate (eGFR), the albumin-to-creatinine ratio (ACR), CD20 levels, IgG levels, and the incidence of infections. Kidney biopsies were performed in 94% of SRNS patients. RTX was administered every 6-9 months, depending on CD20 levels, IgG levels, and the presence of infections. The eGFR and ACR were assessed every 6 months.
Some 31 children were selected for RTX treatment. Overall, 2 experienced severe allergic reactions, leading to their exclusion from the final analysis of 29 children. In the SSNS group, all children achieved and maintained complete remission within 2 years. Remission rates in the SRNS group ranged from 39% (RR 0.78; 95% CI: 16.4-61.4%, NNT 9) at the 6th month to 72% (RR 1.44; 95% CI: 51.5-92.9%) over the 2-year follow-up period due to continuous RTX therapy. The median duration of RTX use was 26.1 months, with a median cumulative dose of 1820 mg/m. Adverse reactions and complications were presented by mild infusion-related reactions in 3 children (10.3%), severe allergic reactions in 2 children (6.2%), hypogammaglobulinemia in 7 children (24%), infections in 3 children (10.3%), severe destructive pneumonia in 1 child, recurrent respiratory infections in 2 children, and neutropenia in 1 child (3.44%).
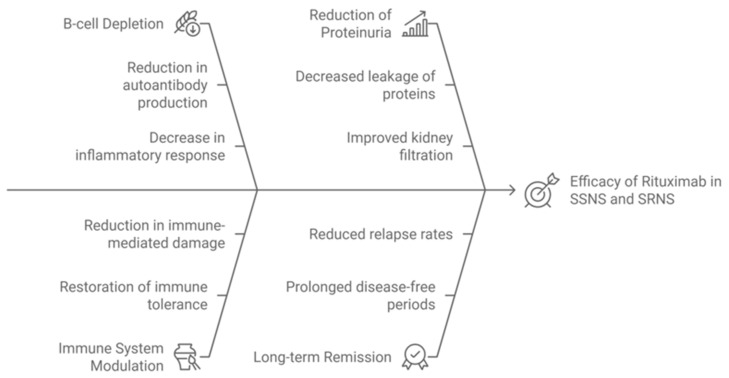
RTX was tolerated well, and proved highly effective as a steroid-sparing agent, offering potential in terms of stopping relapses and minimizing steroid-related side effects. It also demonstrated efficacy in slowing progression in SRNS, indicating potential for use in ACR reduction and renal function restoration, but requires careful use given potential severe allergic reactions and infectious complications. Further studies should focus on long-term cost-effectiveness and deferred side effects.
激素敏感型肾病综合征(SSNS)和激素抵抗型肾病综合征(SRNS)严重影响儿童的生活质量。SSNS频繁复发,SRNS则会进展。国际小儿肾脏病协会(IPNA)指南表明,诸如利妥昔单抗(RTX)之类的单克隆抗体是很有前景的治疗方法。
本研究旨在评估利妥昔单抗治疗SSNS(包括频复发肾病综合征(FRNS)和激素依赖型肾病综合征(SDNS))及SRNS患儿两年随访期的长期疗效和安全性,以促进个体化管理。
我们开展了一项开放标签、多中心、随机且以患者为导向的研究(RICHNESS),纳入3至18岁接受2年持续RTX治疗的SRNS患儿(18例)和SSNS患儿(11例)。主要结局是根据IPNA/KDIGO指南定义的在RTX治疗6、12、18和24个月时的完全/部分缓解(CR/PR);次要结局包括不良事件。关键终点包括估计肾小球滤过率(eGFR)、白蛋白与肌酐比值(ACR)、CD20水平、IgG水平及感染发生率。94%的SRNS患者进行了肾活检。根据CD20水平、IgG水平及是否存在感染,每6至9个月给予一次RTX。每6个月评估一次eGFR和ACR。
约31名儿童被选入RTX治疗组。总体而言,2名儿童出现严重过敏反应,导致其被排除在对29名儿童的最终分析之外。在SSNS组中,所有儿童在2年内均实现并维持完全缓解。由于持续RTX治疗,SRNS组的缓解率在第6个月时为39%(相对危险度0.78;95%置信区间:16.4 - 61.4%,需治疗人数9),在2年随访期内升至72%(相对危险度1.44;95%置信区间:51.5 - 92.9%)。RTX使用的中位持续时间为26.1个月,中位累积剂量为1820mg/m。不良反应和并发症包括3名儿童(10.3%)出现轻度输液相关反应、2名儿童(6.2%)出现严重过敏反应、7名儿童(24%)出现低丙种球蛋白血症、3名儿童(10.3%)出现感染、1名儿童出现严重坏死性肺炎、2名儿童出现反复呼吸道感染以及1名儿童(3.44%)出现中性粒细胞减少症。
RTX耐受性良好,作为一种激素替代药物被证明非常有效,在阻止复发和将激素相关副作用降至最低方面具有潜力。它在减缓SRNS进展方面也显示出疗效,表明在降低ACR和恢复肾功能方面具有应用潜力,但鉴于可能出现的严重过敏反应和感染并发症,需要谨慎使用。进一步的研究应关注长期成本效益和延迟出现的副作用。