Piramide F, Sica M, Fondello G, Mesterca G, Ferrando L, Ziani N, Ortenzi M, Grosso G, Desana B, Frattoni P, De Cillis S, Piana A, Amparore D, Checcucci E, Fiori C, Cirillo S, Porpiglia F, Manfredi M
Department of Oncology, Division of Urology, University of Turin, San Luigi Gonzaga Hospital, 10043 Turin, Italy.
Department of Surgery, Division of Urology, IRCCS Candiolo Cancer Institute, 10060 Turin, Italy.
J Clin Med. 2024 Nov 18;13(22):6955. doi: 10.3390/jcm13226955.
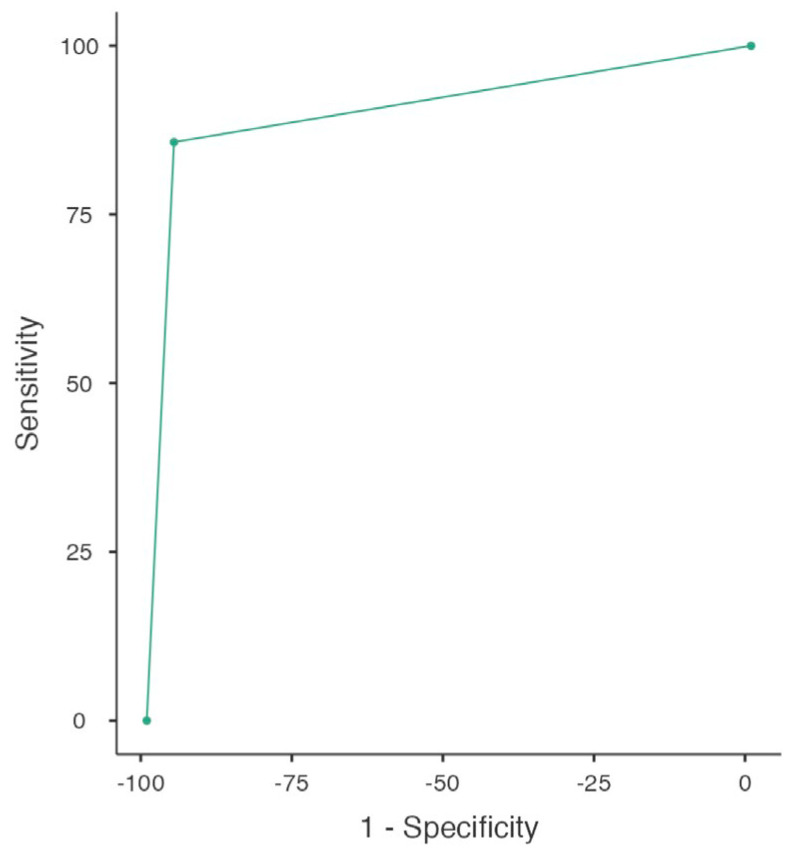
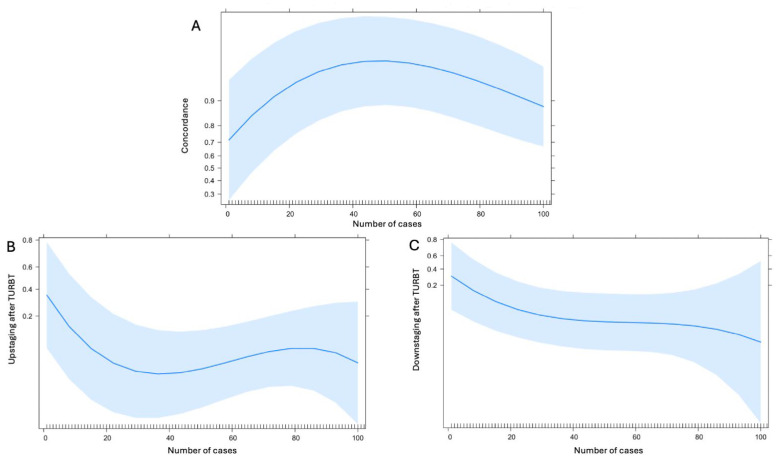
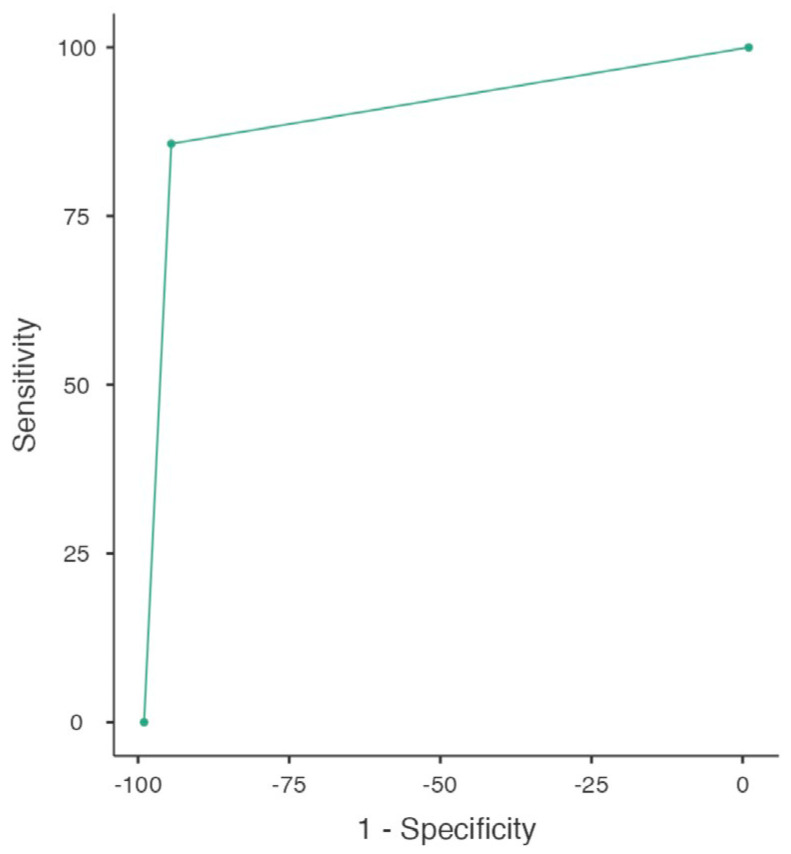
: Nowadays, thanks to the introduction of the VI-RADS scoring system, mpMRI has shown promising results in pre-TURBT assessment of muscular invasiveness of BCa, even if its application in everyday practice is still limited. This might be due to a lack in the literature about the learning curve of radiologists and about the characteristics of the exam. With the aim to reduce scan time and patient discomfort while maintaining diagnostic accuracy, bpMRI has been introduced as a possible alternative to mpMRI in this group of patients. This study reports a single-center experience using mpMRI and the VI-RADS scoring system to differentiate NMIBC from MIBC. The primary aim of the study is to assess diagnostic accuracy of mpMRI using the VI-RADS scoring system. The secondary aim is to evaluate the learning curve of an experienced mpMRI radiologist. Additionally, we perform a retrospective assessment of the same group of patients evaluating only DWIs and T2-weighted images, as they underwent bpMRI, to compare the performance of mpMRI and bpMRI. From 11/2021 to 11/2023, patients with suspected newly diagnosed BCa were enrolled in this prospective study. All patients underwent mpMRI prior to TURBT in a highly specialized radiology center for MRI. According to VI-RADS, a cutoff of ≥3 was assumed to define MIBC. Histological TURBT reports were compared with preoperative VI-RADS scores to assess the accuracy of mpMRI in discriminating between NMIBC and MIBC. Furthermore, to assess the learning curve of the reading radiologist we analyzed the rate of patients correctly classified as MIBC at MRI. Finally, we evaluated the performance of a hypothetic biparametric MRI in classifying our cohort according to VI-RADS score and compared it with mpMRI performance by using DeLong's test. Data analysis was performed using Jamovi software v.2.3 and R software v.4.2.1. A total of 133 patients were enrolled. mpMRI showed sensitivity and specificity of 86% (95% confidence interval [CI]: 64-97) and 95% (95% CI: 89-98), respectively. The learning curve analysis of the reading radiologist showed that the rate of patients correctly classified as MIBC rapidly increases reaching its plateau after 40 cases. The hypothetic bpMRI showed a sensitivity of 76% (95% CI: 53-92) and a specificity of 93% (95% CI: 86-97), with no significant difference with mpMRI performance ( = 0.10). Our study confirms the effectiveness of MRI, particularly with the VI-RADS scoring system, in differentiating NMIBC from MIBC. The learning curve analysis underscores the importance of radiologist training in optimizing diagnostic accuracy. Future research should focus on enhancing the sensitivity of bpMRI and further validating these findings in larger and multicentric studies.
如今,由于VI-RADS评分系统的引入,mpMRI在BCa肌层浸润性的TURBT前评估中显示出了有前景的结果,即便其在日常实践中的应用仍然有限。这可能是由于文献中缺乏关于放射科医生学习曲线以及该检查特征的内容。为了在保持诊断准确性的同时减少扫描时间和患者不适,bpMRI已被引入作为这组患者中mpMRI的一种可能替代方案。本研究报告了一项使用mpMRI和VI-RADS评分系统区分NMIBC和MIBC的单中心经验。该研究的主要目的是使用VI-RADS评分系统评估mpMRI的诊断准确性。次要目的是评估一位经验丰富的mpMRI放射科医生的学习曲线。此外,我们对同一组患者进行回顾性评估,这些患者因接受bpMRI仅评估了DWI和T2加权图像,以比较mpMRI和bpMRI的性能。从2021年11月至2023年11月,疑似新诊断BCa的患者被纳入这项前瞻性研究。所有患者在一个高度专业化的MRI放射科中心接受TURBT前的mpMRI检查。根据VI-RADS,假定≥3的临界值来定义MIBC。将组织学TURBT报告与术前VI-RADS评分进行比较,以评估mpMRI在区分NMIBC和MIBC方面的准确性。此外,为了评估阅片放射科医生的学习曲线,我们分析了在MRI时被正确分类为MIBC的患者比例。最后,我们评估了假设的双参数MRI根据VI-RADS评分对我们队列进行分类的性能,并使用DeLong检验将其与mpMRI性能进行比较。使用Jamovi软件v.2.3和R软件v.4.2.1进行数据分析。总共纳入了133例患者。mpMRI的敏感性和特异性分别为86%(95%置信区间[CI]:64 - 97)和95%(95%CI:89 - 98)。阅片放射科医生的学习曲线分析表明,被正确分类为MIBC的患者比例在40例之后迅速上升并达到平台期。假设的bpMRI的敏感性为76%(95%CI:53 - 92),特异性为93%(95%CI:86 - 97),与mpMRI性能无显著差异( = 0.10)。我们的研究证实了MRI,特别是结合VI-RADS评分系统,在区分NMIBC和MIBC方面的有效性。学习曲线分析强调了放射科医生培训在优化诊断准确性方面的重要性。未来的研究应专注于提高bpMRI的敏感性,并在更大规模的多中心研究中进一步验证这些发现。