Medical University Department, Kantonsspital Aarau, Aarau, Switzerland.
IHU PROMETHEUS, Raymond Poincaré Hospital (APHP), INSERM, Université Paris Saclay Campus Versailles, Paris, France.
BMC Cancer. 2024 Nov 28;24(1):1467. doi: 10.1186/s12885-024-13160-2.
Use of serum procalcitonin (PCT), an inflammatory biomarker for bacterial infections, has shown promising results for early stopping antibiotic treatment among patients with respiratory infections and sepsis. There is need for additional data regarding effectiveness and safety of this concept among patients with cancer.
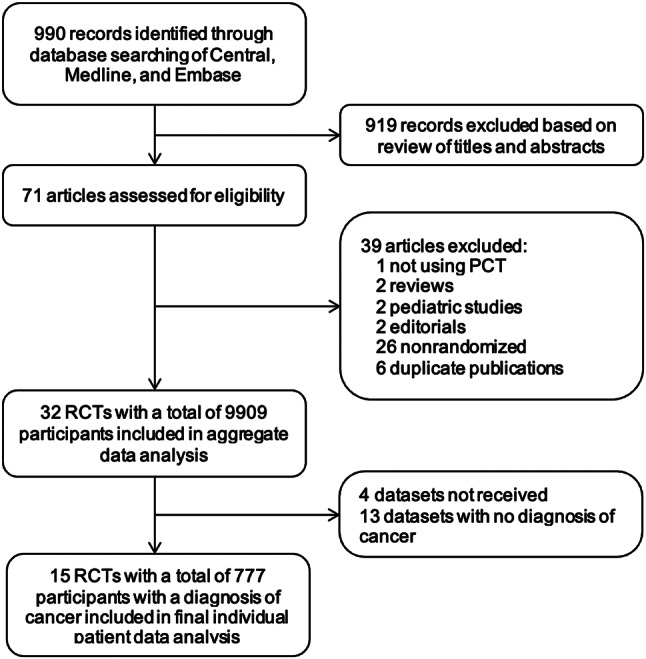
Individual data of patients with a documented diagnosis of cancer and proven or suspected respiratory infection and/or sepsis were extracted from previous trials where adult patients were randomized to receive antibiotic treatment based on a PCT protocol or usual care (control group). The primary efficacy and safety endpoints were antibiotic exposure and 28-day all-cause mortality.
This individual-patient data meta-analysis included 777 patients with a diagnosis of cancer from 15 randomized-controlled trials. Regarding efficacy, there was a 18% reduction in antibiotic exposure in patients randomized to PCT-guided care compared to usual care ([days] 8.2 ± 6.6 vs. 9.8 ± 7.3; adjusted difference, - 1.77 [95% CI, - 2.74 to - 0.80]; p < 0.001). Regarding safety, there were 72 deaths in 379 patients in the PCT-guided group (19.0%) compared to 91 deaths in 398 participants in the usual care group (22.9%) resulting in an adjusted OR of 0.78 (95% CI, 0.60 to 1.02). A subgroup analysis showed a significant reduction in mortality in patients younger than 70 years (adjusted OR, 0.58 [95% CI, 0.40 to 0.86]).
Result of this individual patient meta-analysis from 15 previous trials suggests that among patients with cancer and suspected or proven respiratory infection or sepsis, use of PCT to guide antibiotic treatment decisions results in reduced antibiotic exposure with a possible reduction in mortality, particularly among younger patients.
血清降钙素原(PCT)是一种用于细菌感染的炎症生物标志物,其在呼吸道感染和脓毒症患者中早期停止抗生素治疗方面显示出了良好的效果。对于癌症患者,还需要更多关于该概念的有效性和安全性的数据。
从之前的试验中提取了有明确癌症诊断、确诊或疑似呼吸道感染和/或败血症的患者的个人数据,这些试验将成年患者随机分配接受基于 PCT 方案或常规护理(对照组)的抗生素治疗。主要疗效和安全性终点为抗生素暴露和 28 天全因死亡率。
这项个体患者数据荟萃分析纳入了来自 15 项随机对照试验的 777 例癌症患者。在疗效方面,与常规护理相比,接受 PCT 指导护理的患者抗生素暴露减少了 18%([天]8.2±6.6 vs. 9.8±7.3;调整差异,-1.77[95%置信区间,-2.74 至 -0.80];p<0.001)。在安全性方面,PCT 指导组 379 例患者中有 72 例死亡(19.0%),而常规护理组 398 例患者中有 91 例死亡(22.9%),校正后 OR 为 0.78(95%置信区间,0.60 至 1.02)。亚组分析显示,70 岁以下患者的死亡率显著降低(校正后 OR,0.58[95%置信区间,0.40 至 0.86])。
来自 15 项先前试验的个体患者荟萃分析结果表明,在癌症患者中,对于疑似或确诊的呼吸道感染或败血症患者,使用 PCT 指导抗生素治疗决策可减少抗生素暴露,并可能降低死亡率,特别是在年轻患者中。