Department of Medicine, Geneva University Hospitals, Geneva, Switzerland
Department of Medicine, Geneva University Hospitals, Geneva, Switzerland.
BMJ Open. 2024 Nov 28;14(11):e084825. doi: 10.1136/bmjopen-2024-084825.
Sickle cell disease (SCD) is one of the most common genetic diseases in the world, annually affecting approximately 310 000 births and causing >100 000 deaths. Vaso-occlusive crisis (VOC) is the most frequent complication of SCD, leading to bone pain, thoracic pain (acute chest syndrome) and/or abdominal spasms. It is the main cause of mortality in patients with SCD, reducing life expectancy. Hyperbaric oxygen therapy (HBOT) is a safe and well-established method of increasing tissue oxygen delivery immediately by up to 10-fold to 20-fold. In the context of VOC, HBOT has the potential to limit sickling. A previous pilot study of nine patients showed the safety and potential benefits of HBOT on VOC-induced pain. Our study aimed to assess the clinical safety and effectiveness of HBOT for treating VOC, its biological mechanisms of actions and its cost-effectiveness.
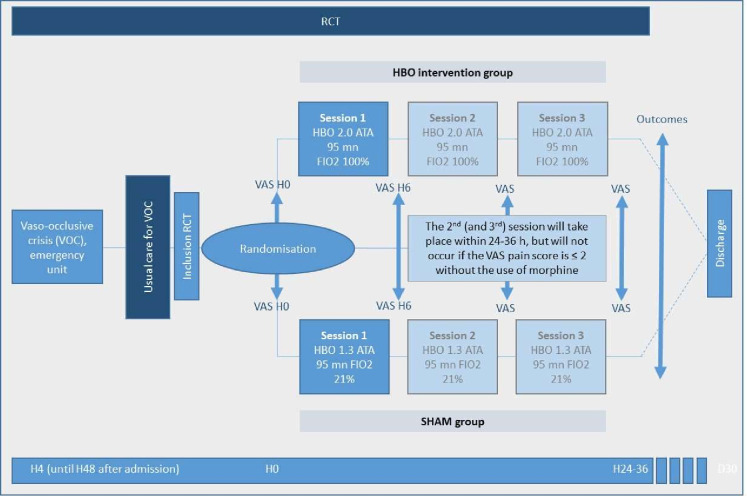
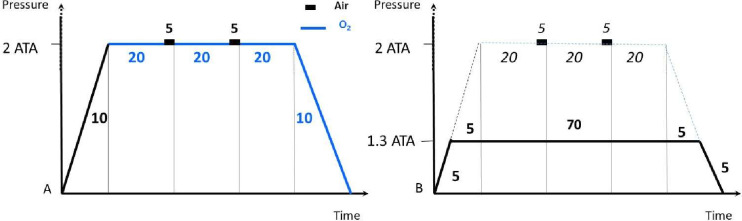
This is a multicentric, triple-blinded, randomised controlled trial. Patients aged 8 years or above with a diagnosed major form of SCD, presenting at one of the participating centres' emergency departments (EDs) with a VOC requiring level 3 analgesia (according to WHO definition), will be eligible. Exclusion criteria are pregnancy, mechanical ventilation, previous history of stroke or prior transcranial Doppler ultrasound anomaly, contraindication to HBOT and the need for above 2 L/min of oxygen. All patients will receive the usual care for VOCs, including hydration, analgesics, normobaric oxygen therapy and when medically indicated, antibiotic therapy and/or transfusions. Within 24 hours of their arrival in the ED (or longer in specific cases), and after obtaining informed consent, patients will be randomised into the HBOT intervention group (2.0 atmosphere absolute (ATA), 90 min, FIO=1) or the sham group (1.3 ATA, 90 min, FIO=0.21). After their first HBOT session, patients will return to their acute-care ward. Patients in both arms will undergo a second and third session within 24-36 hours of the first, unless their Visual Analogue Scale (VAS)-pain is ≤2 without use of level 3 analgesics. The difference in the pain-VAS before and after HBOT and other outcomes will be compared between the intervention and sham groups. Our composite primary outcome will be (1) the change in global VAS-pain 6 hours after initiation of HBOT; (2) the number of patients with a VAS-pain score >4 and/or a morphine dosage >1 mg/hour intravenous after the HBOT/sham session. Other outcomes to be reported are morphine usage, length of stay, biological parameters, satisfaction, complications and cost.
Ethical approval CER Geneva 2019-01707 (last submission V.5.1, 06.15.2023). The results of the studies will be disseminated by several media, including publications in peer-reviewed international medical journals, and presentations at national and/or international conferences.
NCT04978116.
镰状细胞病(SCD)是世界上最常见的遗传性疾病之一,每年影响约 310000 例新生儿,并导致超过 100000 人死亡。血管阻塞危象(VOC)是 SCD 最常见的并发症,导致骨痛、胸痛(急性胸痛综合征)和/或腹部痉挛。它是 SCD 患者死亡的主要原因,降低了预期寿命。高压氧治疗(HBOT)是一种安全且成熟的方法,可立即将组织氧输送增加 10 到 20 倍。在 VOC 的情况下,HBOT 有可能限制镰变。以前对 9 名患者的一项试点研究表明,HBOT 对 VOC 诱导的疼痛具有安全性和潜在益处。我们的研究旨在评估 HBOT 治疗 VOC 的临床安全性和有效性、其生物学作用机制及其成本效益。
这是一项多中心、三盲、随机对照试验。年龄在 8 岁或以上、患有确诊的主要形式 SCD、在参与中心之一的急诊部(ED)出现需要 3 级镇痛(根据世界卫生组织的定义)的 VOC 的患者将符合条件。排除标准是妊娠、机械通气、既往中风史或先前经颅多普勒超声异常、HBOT 禁忌证以及需要 2 升/分钟以上的氧气。所有患者都将接受 VOC 的常规护理,包括补液、镇痛剂、常压氧疗以及在医学上需要时,抗生素治疗和/或输血。在患者到达 ED 的 24 小时内(或在特定情况下更长时间),并在获得知情同意后,患者将被随机分配到 HBOT 干预组(2.0 绝对大气压(ATA),90 分钟,FIO=1)或假组(1.3 ATA,90 分钟,FIO=0.21)。在他们的第一次 HBOT 治疗后,患者将返回他们的急性护理病房。如果患者的视觉模拟量表(VAS)疼痛≤2 且未使用 3 级镇痛剂,则两组患者将在第一次治疗后 24-36 小时内进行第二次和第三次治疗。干预组和假组之间将比较 HBOT 前后疼痛 VAS 的差异和其他结果。我们的复合主要结果将是:(1)HBOT 开始后 6 小时的全球 VAS 疼痛变化;(2)HBOT/假治疗后 VAS 疼痛评分>4 和/或吗啡剂量>1 毫克/小时静脉注射的患者人数。其他要报告的结果是吗啡使用、住院时间、生物学参数、满意度、并发症和成本。
日内瓦 CER 伦理批准 2019-01707(最后提交 V.5.1,2023 年 6 月 15 日)。研究结果将通过多种媒体传播,包括在同行评议的国际医学期刊上发表文章,以及在国内和/或国际会议上发表演讲。
NCT04978116。