Haddad T S, Bokhorst J M, Berger M D, Dobbelsteen L V D, Simmer F, Ciompi F, Galon J, Laak J V D, Pagès F, Zlobec I, Lugli A, Nagtegaal I D
Radboud University Medical Center, Nijmegen, Netherlands.
Department of Medical Oncology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
J Transl Med. 2024 Dec 2;22(1):1090. doi: 10.1186/s12967-024-05818-z.
Tumor Budding (TB) and Immunoscore are independent prognostic markers in colon cancer (CC). Given their respective representation of tumor aggressiveness and immune response, we examined their combination in association with patient disease-free survival (DFS) in pTNM stage I-III CC.
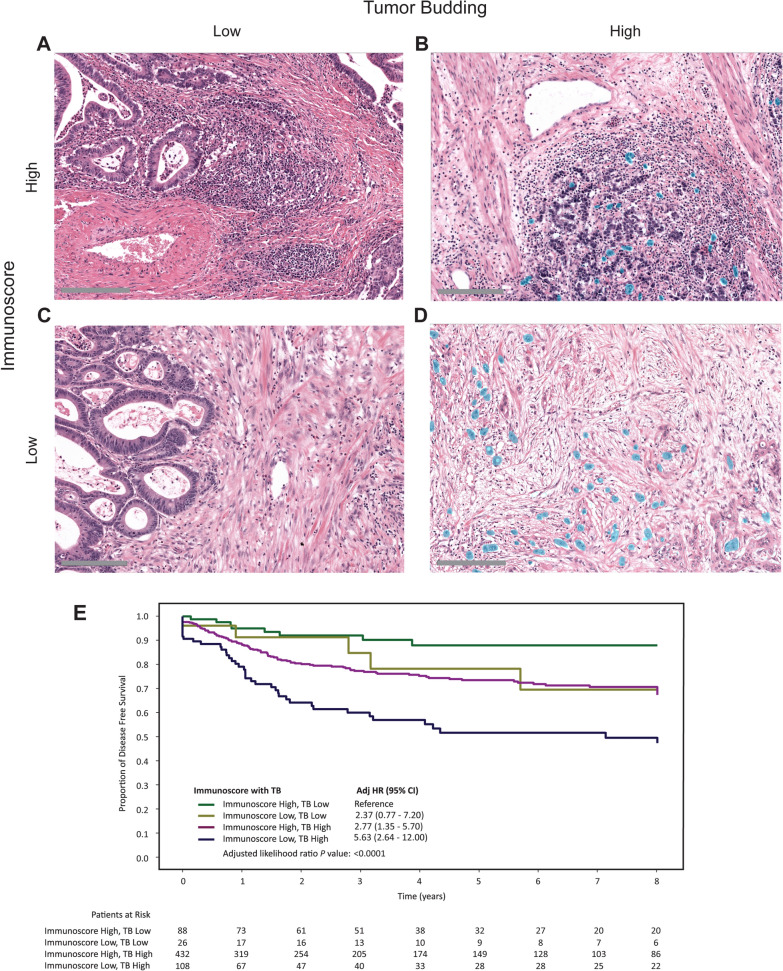
In a series of pTNM stage I-III CCs (n = 654), the Immunoscore was computed and TB detected automatically using a deep learning network. Two-tiered systems for both biomarkers were used with cut-offs of 25% and ten buds for Immunoscore and TB according to clinical guidelines, respectively. Associations of Immunoscore with TB with 5-year DFS were examined using Kaplan-Meier survival analysis in addition to multivariable modeling and relative contribution analysis using Cox regression.
Immunoscore and TB independently are prognostic with hazard ratio (HR) = 2.0, 95% confidence interval (CI) 1.4-2.8 and HR 2.5, with 95% CI 1.4-4.5, respectively; P value < 0.0001. By combining Immunoscore with TB, patients with Immunoscore Low, TB High tumors had a significantly poorer DFS (HR 5.6, 95% CI 2.6-12.0; P value < 0.0001) than those with Immunoscore High, TB Low tumors. The combined Immunoscore with TB score was independently prognostic (P value = 0.009) in comparison to N-stage, T-stage, and MSI. Immunoscore with TB had the highest relative contribution (35%) to DFS in pTNM stage I-II CCs.
The association of Immunoscore and TB with patient survival suggests that both biomarkers are complementary and should be interpreted in combination to identify high-risk Stage I-II patients who should be considered for adjuvant therapy or further diagnostic testing.
肿瘤芽生(TB)和免疫评分是结肠癌(CC)的独立预后标志物。鉴于它们分别代表肿瘤侵袭性和免疫反应,我们研究了它们在pTNM I - III期CC患者无病生存期(DFS)中的联合情况。
在一系列pTNM I - III期CC患者(n = 654)中,计算免疫评分并使用深度学习网络自动检测TB。根据临床指南,两种生物标志物均采用两级系统,免疫评分和TB的临界值分别为25%和10个芽。除了使用Cox回归进行多变量建模和相对贡献分析外,还采用Kaplan - Meier生存分析研究免疫评分与TB与5年DFS的关联。
免疫评分和TB分别具有独立的预后价值,风险比(HR)分别为2.0,95%置信区间(CI)1.4 - 2.8和HR 2.5,95% CI 1.4 - 4.5;P值<0.0001。通过将免疫评分与TB相结合,免疫评分低、TB高的肿瘤患者的DFS明显比免疫评分高、TB低的肿瘤患者差(HR 5.6,95% CI 2.6 - 12.0;P值<0.0001)。与N分期、T分期和微卫星高度不稳定(MSI)相比,免疫评分与TB评分的联合具有独立的预后价值(P值 = 0.009)。在pTNM I - II期CC中,免疫评分与TB对DFS的相对贡献最高(35%)。
免疫评分和TB与患者生存的关联表明,这两种生物标志物具有互补性,应结合起来解释,以识别应考虑辅助治疗或进一步诊断检测的高危I - II期患者。