Chen Yang, Huang Bi, Calvert Peter, Liu Yang, Gue Ying, Gupta Dhiraj, McDowell Garry, Azariah Jinbert Lordson, Namboodiri Narayanan, Unni Govindan, Balagopalan Jayagopal Pathiyil, Lip Gregory Yoke Hong, Gopalan Bahuleyan Charantharayil
Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool Heart and Chest Hospital, Liverpool, United Kingdom.
Department of Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, United Kingdom.
Lancet Reg Health Southeast Asia. 2024 Nov 14;31:100507. doi: 10.1016/j.lansea.2024.100507. eCollection 2024 Dec.
Patients with atrial fibrillation (AF) frequently experience multimorbidity. Cluster analysis, a machine learning method for classifying patients with similar phenotypes, has not yet been used in South Asian AF patients.
The Kerala Atrial Fibrillation Registry is a prospective multicentre cohort study in Kerala, India, and the largest prospective AF registry in South Asia. Hierarchical clustering was used to identify different phenotypic clusters. Outcomes were all-cause mortality, major adverse cardiovascular events (MACE), and composite bleeding events within one-year follow-up.
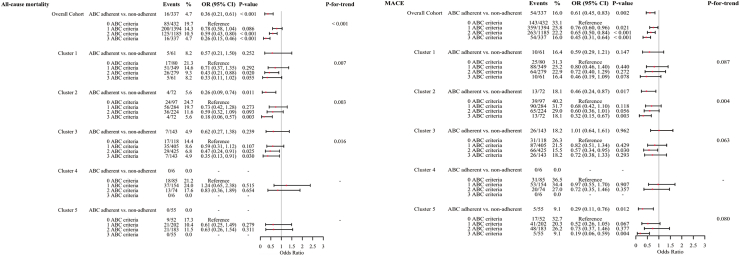
3348 patients were included (median age 65.0 [56.0-74.0] years; 48.8% male; median CHADS-VASc 3.0 [2.0-4.0]). Five clusters were identified. Cluster 1: patients aged ≤65 years with rheumatic conditions; Cluster 2: patients aged >65 years with multi-comorbidities, suggestive of cardiovascular-kidney-metabolic syndrome; Cluster 3: patients aged ≤65 years with fewer comorbidities; Cluster 4: heart failure patients with multiple comorbidities; Cluster 5: male patients with lifestyle-related risk factors. Cluster 1, 2 and 4 had significantly higher MACE risk compared to Cluster 3 (Cluster 1: OR 1.36, 95% CI 1.08-1.71; Cluster 2: OR 1.79, 95% CI 1.42-2.25; Cluster 4: OR 1.76, 95% CI 1.31-2.36). The results for other outcomes were similar. Atrial fibrillation Better Care (ABC) pathway in the whole cohort was low (10.1%), especially in Cluster 4 (1.9%). Overall adherence to the ABC pathway was associated with reduced all-cause mortality (OR 0.26, 95% CI 0.15-0.46) and MACE (OR 0.45, 95% CI 0.31-0.46), similar trends were evident in different clusters.
Cluster analysis identified distinct phenotypes with implications for outcomes. There was poor ABC pathway adherence overall, but adherence to such integrated care was associated with improved outcomes.
Kerala Chapter of Cardiological Society of India.
心房颤动(AF)患者常伴有多种疾病。聚类分析是一种对具有相似表型的患者进行分类的机器学习方法,尚未应用于南亚AF患者。
喀拉拉邦心房颤动登记处是印度喀拉拉邦的一项前瞻性多中心队列研究,也是南亚最大的前瞻性AF登记处。采用层次聚类法识别不同的表型聚类。观察指标为全因死亡率、主要不良心血管事件(MACE)和随访1年内的复合出血事件。
纳入3348例患者(中位年龄65.0[56.0 - 74.0]岁;48.8%为男性;CHADS - VASc中位数为3.0[2.0 - 4.0])。识别出五个聚类。聚类1:年龄≤65岁的风湿性疾病患者;聚类2:年龄>65岁的多合并症患者,提示心血管 - 肾脏 - 代谢综合征;聚类3:年龄≤65岁且合并症较少的患者;聚类4:患有多种合并症的心力衰竭患者;聚类5:具有生活方式相关危险因素的男性患者。与聚类3相比,聚类1、2和4的MACE风险显著更高(聚类1:OR 1.36,95%CI 1.08 - 1.71;聚类2:OR 1.79,95%CI 1.42 - 2.25;聚类4:OR 1.76,95%CI 1.31 - 2.36)。其他观察指标的结果相似。整个队列中心房颤动更佳照护(ABC)路径的依从性较低(10.1%),尤其是在聚类4中(1.9%)。总体上对ABC路径的依从性与全因死亡率降低(OR 0.26,95%CI 0.15 - 0.46)和MACE降低(OR 0.45,95%CI 0.31 - 0.46)相关,在不同聚类中也有类似趋势。
聚类分析识别出了对预后有影响的不同表型。总体上ABC路径依从性较差,但坚持这种综合照护与改善预后相关。
印度心脏病学会喀拉拉邦分会