Yoshida Tsukasa, Takeda Jun, Ishii Sumire, Matsushita Masakazu, Tamura Naoto, Itakura Atsuo
Department of Obstetrics and Gynecology, Juntendo University Faculty of Medicine, Tokyo, Japan.
Department of Internal Medicine and Rheumatology, Juntendo University School of Medicine, Tokyo, Japan.
PLoS One. 2024 Dec 5;19(12):e0303318. doi: 10.1371/journal.pone.0303318. eCollection 2024.
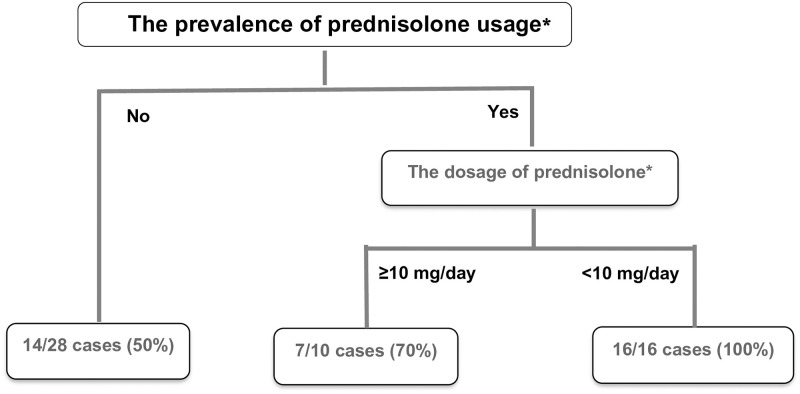
Mixed connective tissue disease (MCTD) predominantly affects women in their reproductive age (30-40 years). This study is aimed to analyze a case series of MCTD-complicated pregnancies. The study design utilized a combined case-series and case-control approach. Pregnant women with MCTD were included and categorized into two groups: the live-birth and non-live birth (encompassing miscarriages at <12 weeks and stillbirths at ≥12 weeks) groups. Primary outcomes included delivery outcomes and factors associated with live births. A total of 57 pregnancies from 34 mothers (median age: 33.0 years) were included. Regarding delivery outcomes, the rates for live birth, miscarriage, and stillbirth were 64.9, 29.8, and 5.3%, respectively. Additionally, the respective rates of preterm delivery, fetal growth restriction (FGR), and small-for-gestational-age (SGA) were 18.9, 18.9, and 27.0%. Higher steroid usage (62.2 vs. 30.0%, p = 0.02) and lower prednisolone dosage in the live birth group (median dose: 7 vs. 10 mg, p = 0.03) were found to be significant factors contributing to live births. MCTD during pregnancy was associated with increased risks of miscarriage, stillbirth, preterm delivery, FGR, and SGA. Notably, low-dose steroid therapy was identified as a contributing factor to successful live births.
混合性结缔组织病(MCTD)主要影响育龄期(30 - 40岁)女性。本研究旨在分析一系列MCTD合并妊娠的病例。研究设计采用了病例系列与病例对照相结合的方法。纳入患有MCTD的孕妇并将其分为两组:活产组和非活产组(包括孕12周前流产和孕12周及以后死产)。主要结局包括分娩结局以及与活产相关的因素。共纳入了来自34位母亲的57次妊娠(中位年龄:33.0岁)。关于分娩结局,活产、流产和死产的发生率分别为64.9%、29.8%和5.3%。此外,早产、胎儿生长受限(FGR)和小于胎龄儿(SGA)的发生率分别为18.9%、18.9%和27.0%。研究发现,活产组更高的类固醇使用量(62.2%对30.0%,p = 0.02)以及更低的泼尼松龙剂量(中位剂量:7 mg对10 mg,p = 0.03)是促成活产的重要因素。孕期MCTD与流产、死产、早产、FGR和SGA风险增加相关。值得注意的是,低剂量类固醇疗法被确定为成功活产的一个促成因素。