Adeoye Oluwatayo, Zheng Guoliang, Onwuemene Oluwatoyosi A
Department of Medicine, St Elizabeth's Medical Center, Boston, MA.
Division of Hematology, Department of Medicine, Virginia Commonwealth University Health, Richmond, VA.
Hematology Am Soc Hematol Educ Program. 2024 Dec 6;2024(1):396-402. doi: 10.1182/hematology.2024000564.
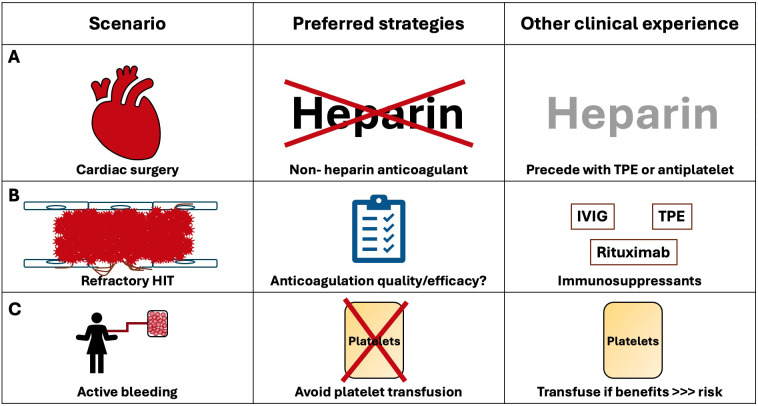
Although heparin-induced thrombocytopenia (HIT) presents management challenges for any population, it adds complexity to the management of certain patient populations, including those undergoing cardiac surgery and those with refractory HIT and/or acute bleeding. For each of these scenarios, we review alternative management strategies when standard therapies-heparin cessation and the initiation of a nonheparin anticoagulant-are either insufficient or not practicable. In patients with HIT undergoing cardiac surgery, we review the clinical experience for heparin reexposure using therapeutic plasma exchange (TPE) or antiplatelet therapy. In patients with refractory HIT despite adequate nonheparin anticoagulation, we address the use of intravenous immune globulin, TPE, and rituximab. Finally, in patients with active bleeding, we discuss bleeding management and the risks associated with platelet transfusion. Although they may facilitate a patient-centered approach, most of these strategies are supported by limited evidence.
尽管肝素诱导的血小板减少症(HIT)给任何人群的管理都带来了挑战,但它给某些患者群体的管理增加了复杂性,包括接受心脏手术的患者以及患有难治性HIT和/或急性出血的患者。对于上述每种情况,当标准治疗方法(停用肝素并开始使用非肝素抗凝剂)不足或不可行时,我们将回顾替代管理策略。对于接受心脏手术的HIT患者,我们回顾了使用治疗性血浆置换(TPE)或抗血小板治疗重新使用肝素的临床经验。对于尽管进行了充分的非肝素抗凝但仍患有难治性HIT的患者,我们讨论了静脉注射免疫球蛋白、TPE和利妥昔单抗的使用。最后,对于有活动性出血的患者,我们讨论了出血管理以及与血小板输注相关的风险。尽管这些策略中的大多数可能有助于采取以患者为中心的方法,但它们大多证据有限。