Agarwal Neeraj, George Daniel J, Klaassen Zachary, Sandin Rickard, Butcher Jake, Ribbands Amanda, Gillespie-Akar Liane, Emir Birol, Russell David, Hong Agnes, Ramaswamy Krishnan, Freedland Stephen J
Huntsman Cancer Institute, University of Utah, Salt Lake City.
Duke Cancer Institute, Duke University School of Medicine, Durham, North Carolina.
JAMA Netw Open. 2024 Dec 2;7(12):e2448707. doi: 10.1001/jamanetworkopen.2024.48707.
Clarifying the underutilization of treatment intensification (TI) for metastatic castration-sensitive prostate cancer (mCSPC) may improve implementation of evidence-based medicine and survival outcomes.
To investigate physicians' beliefs about TI in mCSPC to understand the gap between evidence-based guidelines and clinical practice.
DESIGN, SETTING, AND PARTICIPANTS: This survey study analyzed data from the Adelphi Real World retrospective survey, which comprised physician surveys that were linked to medical record reviews of US adult patients treated for mCSPC between July 2018 and January 2022.
The survey included questions on physician and practice demographics. Physicians completed patient record forms, based on patient medical records with information including patient demographics, clinical characteristics, and patient management. Physicians recalled reasons for prescribing decisions using 48 precoded and open-text responses. Bivariate and multivariable analyses assessed the likelihood of their patients receiving first-line TI; the main outcome was the likelihood of their patients receiving TI using odds ratios (ORs).
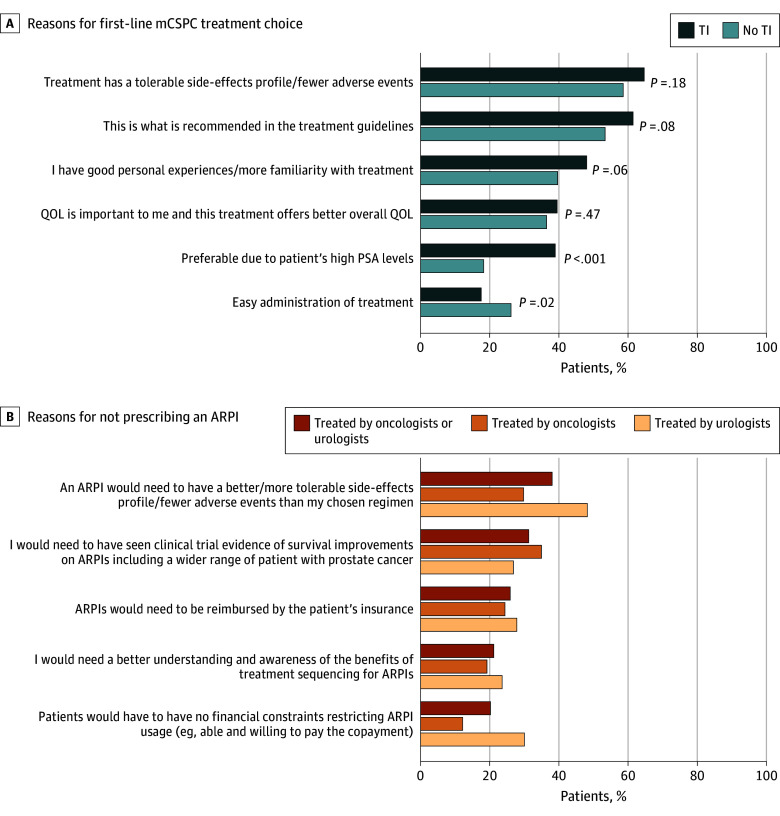
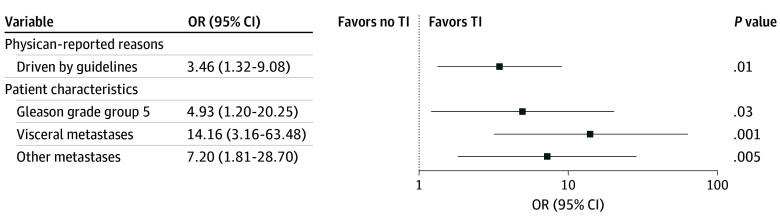
In total, 617 male patients met the analysis criteria (mean [SD] age, 68.6 [8.1] years). Among these patients, 349 (56.6%) were Medicare beneficiaries. Overall, 430 (69.7%) did not receive first-line TI with androgen receptor pathway inhibitors and/or chemotherapy. The 107 US-based physicians' top reasons for treatment choice for their patients were tolerability concerns (TI: 121 [64.7%]; no TI: 252 [58.6%]; P = .18) and following guideline recommendations (TI: 115 [61.5%]; no TI: 230 [53.5%]; P = .08). In the bivariate analysis, physicians seeking to reduce prostate-specific antigen (PSA) by 75% to 100% were more likely to provide first-line TI compared with physicians who aimed to lower PSA by 0% to 49% (OR, 1.63 [95% CI, 1.04-2.56]; P = .03). In the multivariable analysis, patients whose physicians based treatment choice on guidelines were more likely to receive TI than patients whose physicians did not report this reason (OR, 3.46 [95% CI, 1.32-9.08]; P = .01).
The findings of this study, which analyzed data from a medical records-linked clinical practice survey, indicated low rates of first-line TI for mCSPC despite guideline recommendations. Barriers to TI included lack of knowledge about guidelines and published efficacy and safety data. Physicians with greater PSA reduction goals were more likely to use TI. Physician education on treatment guidelines and clinical trial data, while raising expectations for PSA response, may increase rates of first-line TI in mCSPC.
明确转移性去势敏感性前列腺癌(mCSPC)治疗强化(TI)未得到充分利用的情况,可能会改善循证医学的实施及生存结局。
调查医生对mCSPC中TI的看法,以了解循证指南与临床实践之间的差距。
设计、设置和参与者:这项调查研究分析了来自阿德尔菲真实世界回顾性调查的数据,该调查包括与2018年7月至2022年1月期间接受mCSPC治疗的美国成年患者的病历审查相关联的医生调查。
该调查包括有关医生和执业机构人口统计学的问题。医生根据包含患者人口统计学、临床特征和患者管理等信息的患者病历填写患者记录表。医生使用48个预编码和开放文本回复来回溯开处方决策的原因。双变量和多变量分析评估了其患者接受一线TI的可能性;主要结局是使用比值比(OR)评估其患者接受TI的可能性。
共有617名男性患者符合分析标准(平均[标准差]年龄,68.6[8.1]岁)。在这些患者中,349名(56.6%)是医疗保险受益人。总体而言,430名(69.7%)患者未接受雄激素受体通路抑制剂和/或化疗的一线TI。107名美国医生为其患者选择治疗的首要原因是对耐受性的担忧(TI组:121名[64.7%];未接受TI组:252名[58.6%];P = 0.18)以及遵循指南建议(TI组:115名[61.5%];未接受TI组:230名[53.5%];P = 0.08)。在双变量分析中,与旨在将前列腺特异性抗原(PSA)降低0%至49%的医生相比,寻求将PSA降低75%至100%的医生更有可能提供一线TI(OR,1.63[95%CI,1.04 - 2.56];P = 0.03)。在多变量分析中,与医生未报告此原因的患者相比,医生根据指南进行治疗选择的患者更有可能接受TI(OR,3.46[95%CI,1.32 - 9.08];P = 0.01)。
这项分析与病历相关的临床实践调查数据的研究结果表明,尽管有指南建议,但mCSPC的一线TI使用率较低。TI的障碍包括对指南以及已发表的疗效和安全性数据缺乏了解。PSA降低目标更高的医生更有可能使用TI。对医生进行治疗指南和临床试验数据的教育,在提高对PSA反应期望的同时,可能会提高mCSPC一线TI的使用率。