Burke Laura, Hinkson Alexander, Haghnejad Vincent, Jones Rebecca, Parker Richard, Rowe Ian A
Leeds Institute for Medical Research, University of Leeds, Leeds, United Kingdom.
Leeds Liver Unit, Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom.
JHEP Rep. 2024 Oct 9;7(1):101227. doi: 10.1016/j.jhepr.2024.101227. eCollection 2025 Jan.
BACKGROUND & AIMS: Hepatocellular carcinoma (HCC) risk prediction models may provide a more personalised approach to surveillance for HCC among patients with cirrhosis. This systematic review aims to summarise the performance of HCC prediction models in patients with non-viral chronic liver disease.
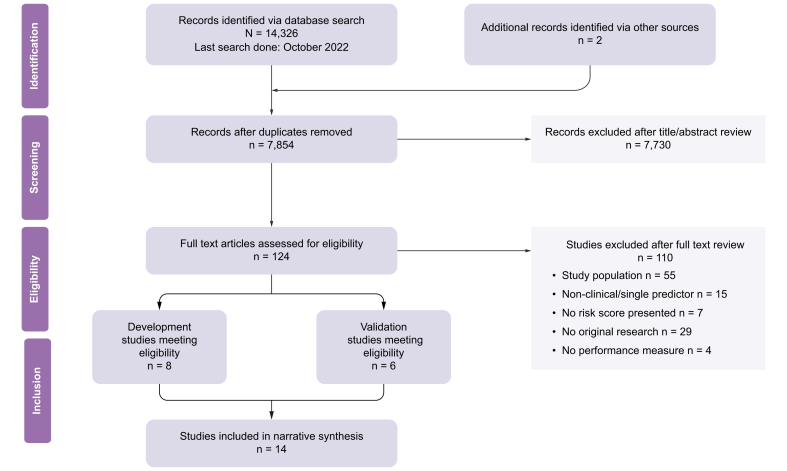
The study was prospectively registered with PROSPERO (ID: CRD42022370078) and reported in accordance with PRISMA guidelines. MEDLINE and Embase databases were searched using a validated search filter for prediction model studies. Two reviewers independently assessed studies for inclusion and risk of bias. Measures of model performance (discrimination and calibration) to assess the risk of HCC at specified time points were identified. A random effects meta-analysis was performed on a subset of studies that reported performance of the same model.
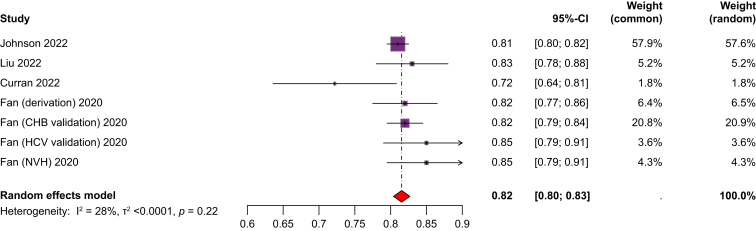
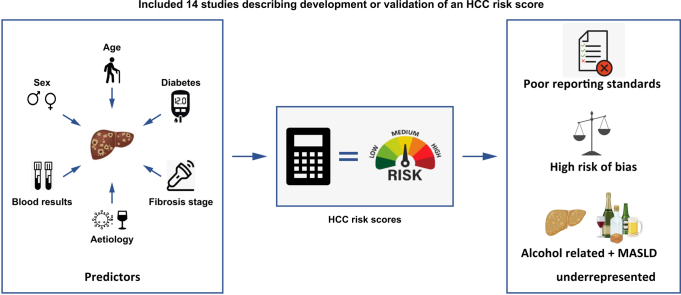
A total of 7,854 studies were identified. After review, 14 studies with a total of 94,014 participants were included; 45% of patients had viral hepatitis, 27% ALD (alcohol-related liver disease) and 19% MASLD (metabolic dysfunction-associated steatotic liver disease). Follow-up ranged from 15.1-138 months. Only one model was developed using a competing risk approach. Age (7 models) and sex (6 models) were the most frequently included predictors. Model discrimination (AUROC or c-statistic) ranged from 0.61-0.947. Only the 'aMAP' score (age, male sex, albumin, bilirubin, and platelets) had sufficient external validation for quantitative analysis, with a pooled c-statistic of 0.81 (95% CI 0.80-0.83). Calibration was reported in only 9 of 14 studies. All studies were rated at high risk of bias.
Studies describing risk prediction of HCC in non-viral chronic liver disease are poorly reported, have a high risk of bias and do not account for competing risk events. Patients with ALD and MASLD are underrepresented in development and validation cohorts. These factors remain barriers to the clinical utility and uptake of HCC risk models for those with the most common liver diseases.
The recent EASL policy statement emphasises the potential of risk-based surveillance to reduce both hepatocellular carcinoma (HCC)-related deaths and surveillance costs. This study addresses the gap in understanding the performance of current HCC risk models in patients with non-viral liver diseases, reflecting the epidemiological landscape of liver disease in Western countries. In our review of these models we identified several key concerns regarding reporting standards and risk of bias and confirmed that patients with alcohol-related liver disease and metabolic dysfunction-associated steatotic liver disease are underrepresented in model development and validation cohorts. Additionally, most models fail to account for the significant risk of competing events, leading to potential overestimation of true HCC risk. This study highlights these critical issues that may hinder the implementation of risk models in clinical practice and offers key recommendations for future model development studies.
肝细胞癌(HCC)风险预测模型可为肝硬化患者的HCC监测提供更具个性化的方法。本系统评价旨在总结非病毒性慢性肝病患者中HCC预测模型的性能。
该研究已在PROSPERO(注册号:CRD42022370078)进行前瞻性注册,并按照PRISMA指南报告。使用经过验证的预测模型研究检索过滤器对MEDLINE和Embase数据库进行检索。两名评审员独立评估纳入研究及偏倚风险。确定了在特定时间点评估HCC风险的模型性能指标(辨别力和校准度)。对报告同一模型性能的部分研究进行随机效应荟萃分析。
共识别出7854项研究。经审查,纳入了14项研究,共94014名参与者;45%的患者患有病毒性肝炎,27%患有酒精性肝病(ALD),19%患有代谢功能障碍相关脂肪性肝病(MASLD)。随访时间为15.1 - 138个月。仅使用竞争风险方法开发了一个模型。年龄(7个模型)和性别(6个模型)是最常纳入的预测因素。模型辨别力(AUROC或c统计量)范围为0.61 - 0.947。只有“aMAP”评分(年龄、男性、白蛋白、胆红素和血小板)有足够的外部验证用于定量分析,合并c统计量为0.81(95%CI 0.80 - 0.83)。14项研究中只有9项报告了校准情况。所有研究均被评为高偏倚风险。
描述非病毒性慢性肝病中HCC风险预测的研究报告质量差,偏倚风险高,且未考虑竞争风险事件。在开发和验证队列中,ALD和MASLD患者的代表性不足。这些因素仍然是HCC风险模型在最常见肝病患者中临床应用和推广的障碍。
最近的欧洲肝脏研究学会(EASL)政策声明强调了基于风险的监测在降低肝细胞癌(HCC)相关死亡和监测成本方面的潜力。本研究弥补了在了解当前HCC风险模型在非病毒性肝病患者中的性能方面的差距,反映了西方国家肝病的流行病学情况。在对这些模型的综述中,我们发现了几个关于报告标准和偏倚风险的关键问题,并证实酒精性肝病和代谢功能障碍相关脂肪性肝病患者在模型开发和验证队列中的代表性不足。此外,大多数模型未能考虑竞争事件的重大风险,导致可能高估了真正的HCC风险。本研究突出了这些可能阻碍风险模型在临床实践中实施的关键问题,并为未来模型开发研究提供了关键建议。