Bisello Silvia, Malizia Claudio, Mammini Filippo, Galietta Erika, Medici Federica, Mattiucci Gian Carlo, Cellini Francesco, Palloni Andrea, Tagliaferri Luca, Macchia Gabriella, Deodato Francesco, Cilla Savino, Brandi Giovanni, Arcelli Alessandra, Morganti Alessio G
Radiation Oncology, AOU delle Marche, Ancona, Italy.
Nuclear Medicine, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Cancer Med. 2024 Dec;13(23):e70196. doi: 10.1002/cam4.70196.
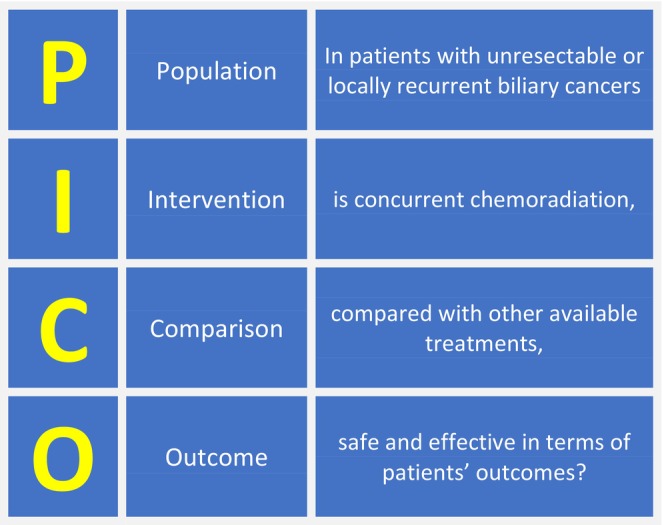
Biliary tract cancers (BTC) are rare and aggressive neoplasms. The current management of locally advanced or unresectable BTC is primarily based on chemotherapy (CHT) alone, linked to a median overall survival (OS) of approximately 12 months. However, international guidelines still consider concurrent chemoradiation (CRT) as an alternative treatment option. This study aims to review the current evidence on "modern" CRT for primary or recurrent unresectable BTC.
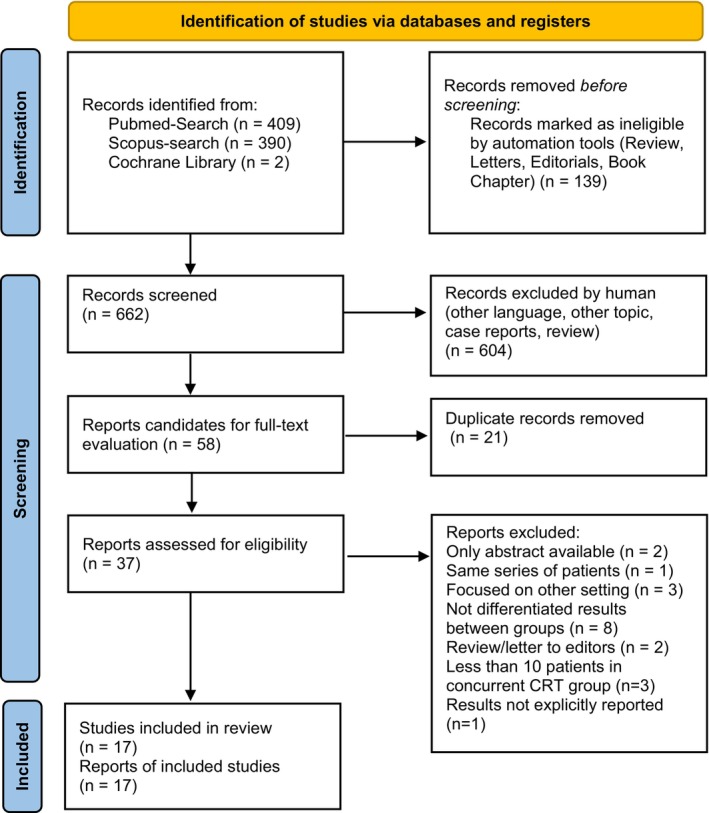
A comprehensive search was conducted on PubMed, Scopus, and Cochrane Library to identify relevant papers. Prospective or retrospective trials reporting outcomes after concurrent CRT of unresectable non-metastatic, primary, or recurrent BTC were included. Only English-written papers published between January 2010 and June 2022 were considered.
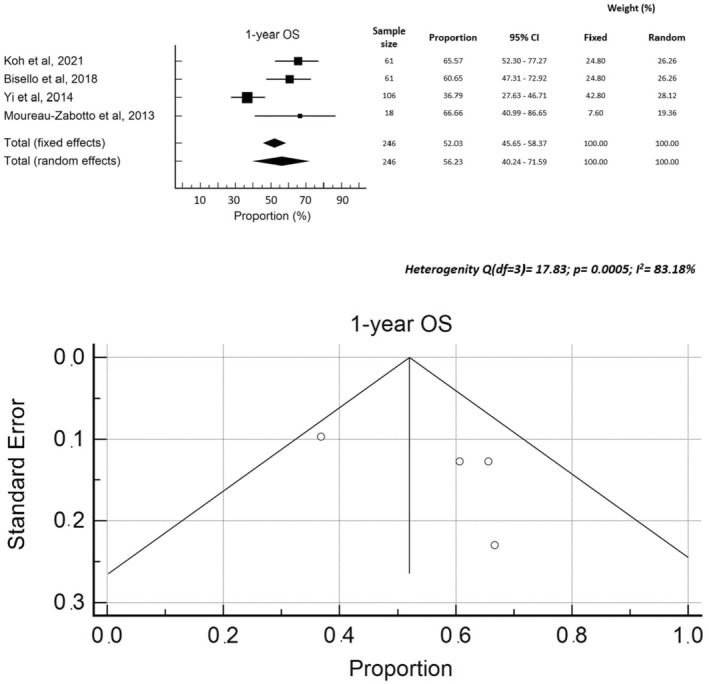
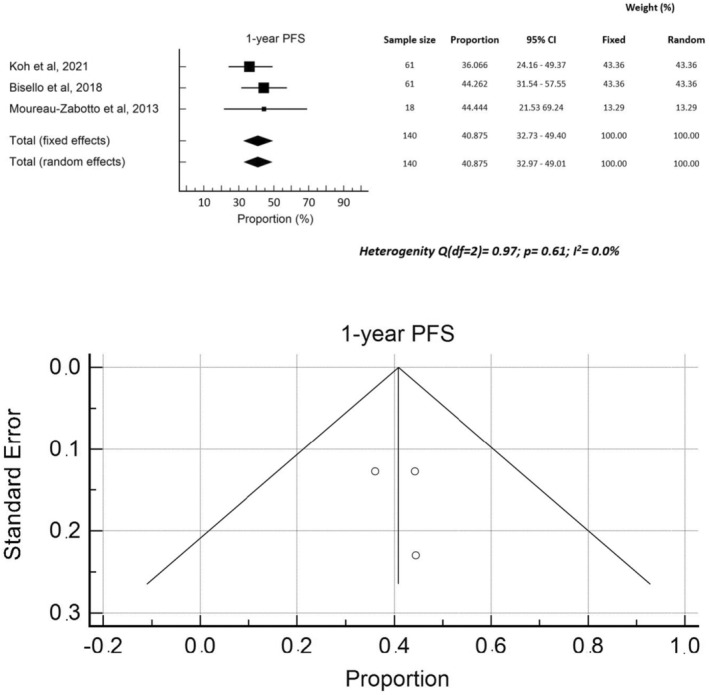
Seventeen papers, comprising a total of 1961 patients, were included in the analysis. Among them, 11 papers focused solely on patients with primary unresectable BTC, while two papers included patients with isolated local recurrences and four papers encompassed both settings. In terms of tumor location, 12 papers included patients with intrahepatic, extrahepatic, and hilar BTC, as well as gallbladder cancer. The median CRT dose delivered was 50.4 Gy (range: 45.0-72.6 Gy) using conventional fractionation. Concurrent CHT primarily consisted of 5-Fluorouracil or Gemcitabine. The pooled rates of 1-year progression-free survival (PFS) and OS were 40.9% and 56.2%, respectively. The median 1- and 2-year OS rates were 63.1% and 29.4%, respectively. Grade ≥3 acute gastrointestinal toxicity ranged from 5.6% to 22.2% (median: 10.9%), while grade ≥3 hematological toxicity ranged from 1.6% to 50.0% (median: 21.7%).
Concurrent CRT is a viable alternative to standard CHT in patients with locally advanced BTC, offering comparable OS and PFS rates, along with an acceptable toxicity profile. However, prospective trials are needed to validate and further explore these findings.
胆道癌(BTC)是罕见且侵袭性强的肿瘤。目前,局部晚期或不可切除的BTC的治疗主要仅基于化疗(CHT),其总体中位生存期(OS)约为12个月。然而,国际指南仍将同步放化疗(CRT)视为一种替代治疗选择。本研究旨在综述关于原发性或复发性不可切除BTC的“现代”CRT的现有证据。
在PubMed、Scopus和Cochrane图书馆进行了全面检索,以识别相关论文。纳入报告不可切除的非转移性、原发性或复发性BTC同步CRT后结局的前瞻性或回顾性试验。仅考虑2010年1月至2022年6月发表的英文论文。
分析纳入了17篇论文,共1961例患者。其中,11篇论文仅关注原发性不可切除BTC患者,2篇论文纳入了孤立局部复发患者,4篇论文涵盖了这两种情况。在肿瘤位置方面,12篇论文纳入了肝内、肝外和肝门部BTC以及胆囊癌患者。采用常规分割时,CRT的中位剂量为50.4 Gy(范围:45.0 - 72.6 Gy)。同步CHT主要由5-氟尿嘧啶或吉西他滨组成。1年无进展生存期(PFS)和OS的合并率分别为40.9%和56.2%。1年和2年OS的中位率分别为63.1%和29.4%。≥3级急性胃肠道毒性范围为5.6%至22.2%(中位值:10.9%),而≥3级血液学毒性范围为1.6%至50.0%(中位值:21.7%)。
对于局部晚期BTC患者,同步CRT是标准CHT的可行替代方案,其OS和PFS率相当,且毒性特征可接受。然而,需要前瞻性试验来验证并进一步探索这些发现。