Madeira Laura Cordeiro, Dalcin Paulo de Tarso, Schuster Gabriele Heinen, Conte Bruna, Wolf Jonas Michel, Schreiber Annia, Rouby Jean-Jacques, Dexheimer-Neto Felippe Leopoldo
. Centro de Terapia Intensiva, Hospital Moinhos de Vento, Porto Alegre (RS) Brasil.
. Programa de Pós-Graduação em Ciências Pneumológicas, Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre (RS) Brasil.
J Bras Pneumol. 2024 Dec 6;50(5):e20240302. doi: 10.36416/1806-3756/e20240302. eCollection 2024.
To compare pre-extubation physiological characteristics and ultrasound variables between patients intubated for COVID-19 compared to a clinical population and those intubated for other reasons.
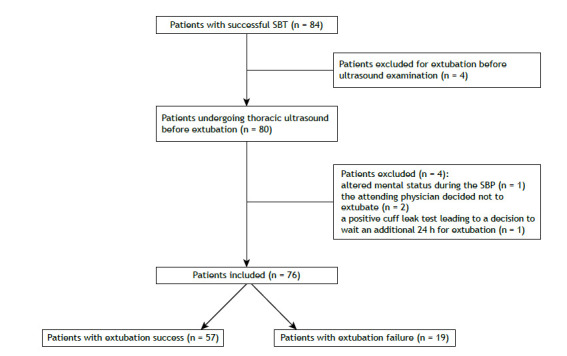
This was a secondary analysis of a prospective cohort study of patients undergoing invasive mechanical ventilation (IMV) for more than 48 h. Patients were divided into two groups: those intubated for COVID-19-induced ARDS and those intubated for other clinical reasons. Ultrasound assessment of lung and diaphragm function was performed before extubation. The results were compared between the two groups of patients.
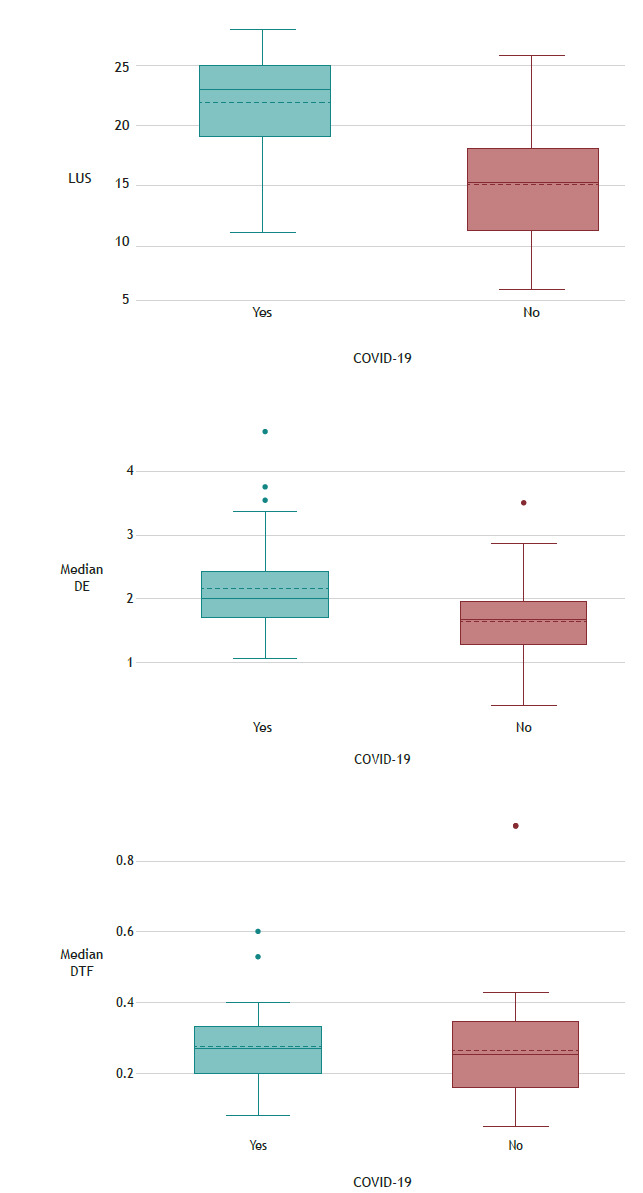
In comparison with the patients without COVID-19, those with the disease were younger (a median age of 58 [46-76] years vs. a median age of 75 [69-85] years; p = 0.01), had fewer comorbidities (a median Charlson Comorbidity Index of 2 [1-4] vs. a median Charlson Comorbidity Index of 5 [4-6]; p < 0.01), and were less severely ill at admission (a median APACHE II score of 9 [8-14] vs. a median APACHE II score of 18 [13-22]; p < 0.01). In addition, the median duration of IMV was longer in the COVID-19 patients (11 [9-23] days vs. 6 [3-8] days; p < 0.01). Although extubation success rates were similar between the COVID-19 and non-COVID-19 groups (22 [71%] vs. 35 [77.8%]), median lung ultrasound score differed between the two groups (23 [18-25] vs. 15 [11-18]; p < 0.01), as did median diaphragmatic excursion (2.1 [1.7-2.4] vs. 1.7 [1.2-2.0]; p < 0.01).
Although patients with COVID-19 requiring ventilatory support are younger and have fewer comorbidities than those intubated for other clinical reasons, they experience longer hospital stays. Although lung ultrasound score can differ between patients with and without COVID-19, these differences do not significantly translate into extubation success rates. Therefore, the utility of ultrasound scores in weaning COVID-19 patients from IMV needs further study.
比较因新型冠状病毒肺炎(COVID-19)插管患者与临床人群以及因其他原因插管患者在拔管前的生理特征和超声变量。
这是一项对接受有创机械通气(IMV)超过48小时患者的前瞻性队列研究的二次分析。患者分为两组:因COVID-19导致的急性呼吸窘迫综合征(ARDS)插管的患者和因其他临床原因插管的患者。在拔管前对肺和膈肌功能进行超声评估。比较两组患者的结果。
与无COVID-19的患者相比,患有该疾病的患者更年轻(中位年龄58[46 - 76]岁 vs. 中位年龄75[69 - 85]岁;p = 0.01),合并症更少(中位查尔森合并症指数2[1 - 4] vs. 中位查尔森合并症指数5[4 - 6];p < 0.01),入院时病情较轻(中位急性生理与慢性健康状况评分系统II(APACHE II)评分为9[8 - 14] vs. 中位APACHE II评分为18[13 - 22];p < 0.01)。此外,COVID-19患者的IMV中位持续时间更长(11[9 - 23]天 vs. 6[3 - 8]天;p < 0.01)。尽管COVID-19组和非COVID-19组的拔管成功率相似(22例[71%] vs. 35例[77.8%]),但两组的中位肺部超声评分不同(23[18 - 25] vs. 15[11 - 18];p < 0.01),中位膈肌移动度也不同(2.1[1.7 - 2.4] vs. 1.7[1.2 - 2.0];p < 0.01)。
尽管需要通气支持的COVID-19患者比因其他临床原因插管的患者更年轻且合并症更少,但他们的住院时间更长。尽管有COVID-19和无COVID-19的患者之间肺部超声评分可能不同,但这些差异并未显著转化为拔管成功率。因此,超声评分在使COVID-19患者从IMV撤机中的效用需要进一步研究。