Barros Guinle Maria Isabel, Johnstone Thomas, Ruiz Colón Gabriela D, Weng Yingjie, Nettnin Ella A, Ratliff John K
Department of Neurosurgery, Stanford University School of Medicine, Stanford, CA, United States.
Quantitative Sciences Unit, Stanford University School of Medicine, Stanford, CA, United States.
N Am Spine Soc J. 2024 Nov 2;20:100565. doi: 10.1016/j.xnsj.2024.100565. eCollection 2024 Dec.
Low back pain (LBP) is the most common medical cause of disability among adults 65 or older. No previous study has characterized health care costs and treatment patterns of LBP among Medicare beneficiaries.
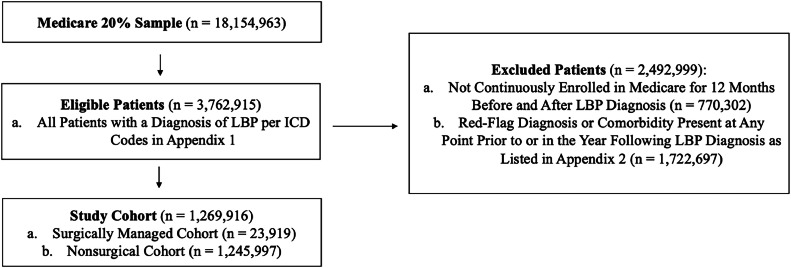
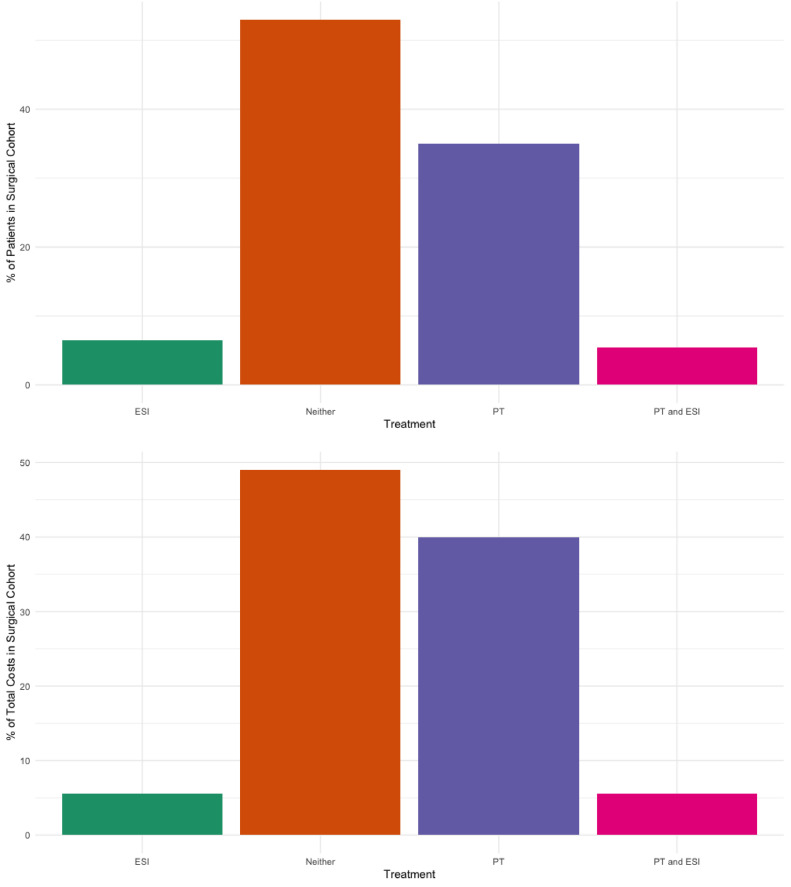
This retrospective cohort study quantifies health care utilization costs among Medicare beneficiaries with newly diagnosed LBP, compares costs between patients managed operatively and nonoperatively, identifies costs associated with treatment guideline nonadherence, and characterizes opioid prescribing patterns. Patients were queried via ICD codes from a 20% random sample of Medicare claims records. Patients with concomitant or previous "red flag" diagnoses, neurological deficits, or diagnoses that could cause nondegenerative LBP were excluded. Total costs of care in the year of diagnosis were calculated and stratified by operative versus nonoperative management. To assess for guideline adherence, utilization and costs of different services were tabulated. Opioid prescription patterns were characterized by quantity, cost, duration, and medication type.
About 1,269,896 patients were identified; 23,919 (1.8%) underwent surgery. These accounted for 7% of the cohort's total cost ($514 million total, $21,496 per person). Patients treated nonoperatively accounted for over $7 billion in costs ($5,880 per person; p<.001). Within the nonoperative cohort, 626,896 (50.3%) patients were nonadherent to current guidelines for conservative management of LBP. Guideline nonadherence increased total annual costs by $4,012 per person ($7,873 for nonadherent vs. $3,861 for adherent patients, p<.001). About 460,867 opioid prescriptions were filled for 303,796 unique patients (23.9%) within 30 days of LBP diagnosis. Within the nonsurgical cohort, patients nonadherent to imaging guidelines were more likely to have an opioid prescription within this window than adherent patients (26.5% vs. 21.2%; p<.001).
Nonoperative management of LBP is associated with significantly lower costs per patient. Early imaging and opioid prescription are significant drivers of excess cost. Adherence to proposed treatment guidelines can save over $2.8 billion in total health care costs.
腰痛(LBP)是65岁及以上成年人中导致残疾的最常见医学原因。此前尚无研究描述医疗保险受益人中腰痛的医疗费用和治疗模式。
这项回顾性队列研究对新诊断为腰痛的医疗保险受益人中的医疗服务利用成本进行了量化,比较了手术治疗和非手术治疗患者的成本,确定了与治疗指南不依从相关的成本,并描述了阿片类药物的处方模式。通过医疗保险理赔记录20%的随机样本中的国际疾病分类代码查询患者。排除伴有或既往有“红旗”诊断、神经功能缺损或可能导致非退行性腰痛的诊断的患者。计算诊断当年的总护理成本,并按手术治疗与非手术治疗进行分层。为评估指南依从性,列出了不同服务的利用情况和成本。阿片类药物处方模式的特征包括数量、成本、持续时间和药物类型。
共识别出约1,269,896名患者;23,919名(1.8%)接受了手术。这些手术患者占队列总成本的7%(总计5.14亿美元,人均21,496美元)。非手术治疗的患者成本超过70亿美元(人均5,880美元;p<0.001)。在非手术队列中,626,896名(50.3%)患者未遵循当前腰痛保守治疗指南。不遵循指南使每人每年的总成本增加4,012美元(不遵循指南的患者为7,873美元,遵循指南的患者为3,861美元,p<0.001)。在腰痛诊断后的30天内,为303,796名(23.9%)不同患者开具了约460,867张阿片类药物处方。在非手术队列中,不遵循影像学指南的患者在此期间开具阿片类药物处方的可能性高于遵循指南的患者(26.5%对21.2%;p<0.001)。
腰痛的非手术治疗与每位患者显著更低的成本相关。早期影像学检查和阿片类药物处方是成本过高的重要驱动因素。遵循建议的治疗指南可节省超过28亿美元的总医疗费用。