Das Anibh M, Ballhausen Diana, Haas Dorothea, Häberle Johannes, Hagedorn Tobias, Janson-Mutsaerts Cecilia, Janzen Nils, Sander Johannes, Freisinger Peter, Karall Daniela, Meyer Uta, Mönch Eberhard, Morlot Susanne, Rosenbaum-Fabian Stefanie, Scholl-Bürgi Sabine, Vom Dahl Stephan, Weinhold Natalie, Zeman Jiri, Lange Karin
Hannover Medical School, Department of Paediatrics, Hannover, Germany.
Pediatric Metabolic Unit, Pediatrics, Woman-Mother-Child Department, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland.
J Inherit Metab Dis. 2025 Jan;48(1):e12824. doi: 10.1002/jimd.12824.
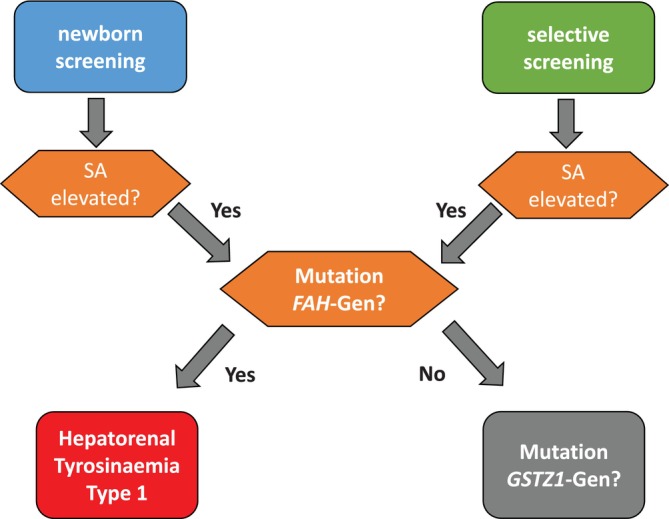
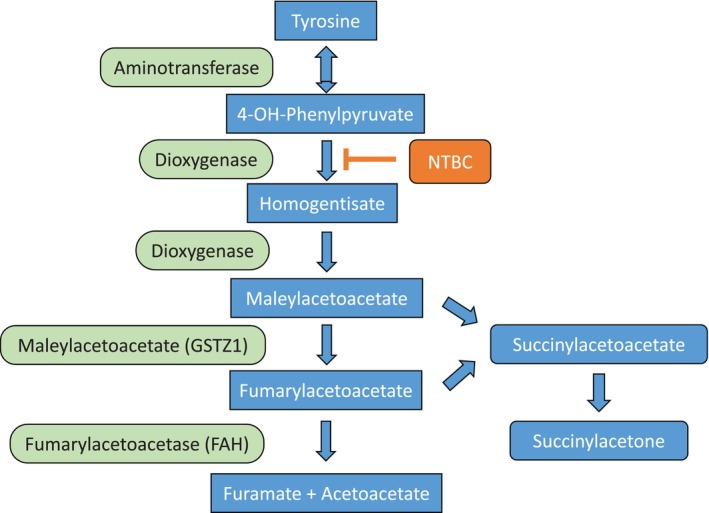
Hepatorenal tyrosinaemia (HT1) is an autosomal recessive disorder of tyrosine degradation resulting in hepatic and renal dysfunction, neurological sequelae may occur in some patients. The use of nitisinone (NTBC) has revolutionised treatment and outcome of this disorder. NTBC has to be combined with a low protein diet. While NTBC modulates the disease course in HT1 patients, several issues are open. Optimal dosage, doses per day, therapeutic range of NTBC concentration, mode of protein restriction and biomarkers are not well defined. HCC and neurocognitive deficits are long-term sequelae. Early diagnosis and treatment are essential to minimise the risk for these complications. Clinical guidance for management of HT1-patients is required. Randomised clinical studies are difficult in the presence of therapeutic options. We discussed these issues in a consensus group of 10 paediatricians, 1 adult hepatologist, 1 geneticist, 2 dieticians, 2 newborn screening specialists with experience in HT1, 1 psychologist and 2 representatives of a patient group from the German-speaking countries (DACH). Recommendations were based on scientific literature and expert opinion, also taking into account recent experience with newborn screening. There was strong consensus that newborn screening using succinylacetone (SA) and early treatment are essential for a good outcome. The dose of NTBC should be as low as possible without losing metabolic control. This has to be accompanied by a low protein diet, in some patients a simplified diet without calculation of protein intake. Specific education and psychosocial support are recommended. Indications for liver transplantation were defined. Monitoring shall include clinical findings, levels of SA, tyrosine, phenylalanine and NTBC in (dried) blood.
肝肾型酪氨酸血症(HT1)是一种常染色体隐性酪氨酸降解障碍疾病,可导致肝肾功能障碍,部分患者可能出现神经后遗症。尼替西农(NTBC)的使用彻底改变了这种疾病的治疗方法和预后。NTBC必须与低蛋白饮食联合使用。虽然NTBC可调节HT1患者的病程,但仍存在一些未解决的问题。NTBC的最佳剂量、每日剂量、治疗浓度范围、蛋白质限制方式和生物标志物尚未明确界定。肝癌和神经认知缺陷是长期后遗症。早期诊断和治疗对于将这些并发症的风险降至最低至关重要。需要针对HT1患者管理的临床指南。在存在多种治疗选择的情况下,进行随机临床研究很困难。我们在一个由10名儿科医生、1名成人肝病专家、1名遗传学家、2名营养师、2名有HT1经验的新生儿筛查专家、1名心理学家以及来自德语国家(DACH)的患者群体的2名代表组成的共识小组中讨论了这些问题。建议基于科学文献和专家意见,同时也考虑到新生儿筛查的最新经验。强烈共识是,使用琥珀酰丙酮(SA)进行新生儿筛查和早期治疗对于取得良好预后至关重要。NTBC的剂量应尽可能低,同时不失去代谢控制。这必须辅以低蛋白饮食,在一些患者中采用无需计算蛋白质摄入量的简化饮食。建议提供特定教育和心理社会支持。明确了肝移植的适应症。监测应包括临床症状、(干)血中SA、酪氨酸、苯丙氨酸和NTBC的水平。