Volpi Sara, Rajah Tanisha, Ali Jason M
Department of Cardiothoracic Surgery, St Thomas' Hospital, London, UK.
School of Cardiovascular Medicine and Sciences, King's College London, London, UK.
J Thorac Dis. 2024 Nov 30;16(11):8088-8102. doi: 10.21037/jtd-24-1112. Epub 2024 Nov 6.
The global prevalence of diabetes mellitus has markedly risen in recent years. Consequently, there has been a rise in the number of patients with diabetes undergoing cardiac surgery. Despite the existence of national and international guidelines to improve surgical outcomes in patients with diabetes, perioperative diabetes management optimisation remains inadequate resulting in these patients experiencing increased rates of surgical morbidity and mortality. This review aims to evaluate outcomes following cardiac surgery in patients with diabetes and assess strategies to enhance preoperative and perioperative optimization and postoperative outcomes.
A comprehensive literature search was performed for articles concerning perioperative management of diabetes in patients undergoing cardiac surgery as well as postoperative complications related to diabetes in addition to interventions utilised to optimize outcomes.
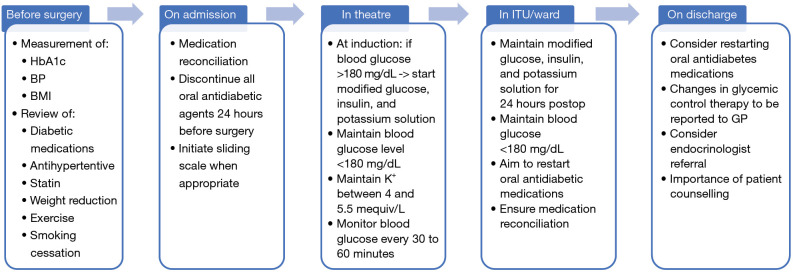
Principle findings were extracted and synthesized. Patients with diabetes undergoing cardiac surgery exhibit increased perioperative complications, higher in-hospital mortality rates and inferior long-term survival. A key facilitator is specifically poor glycemic control, with glycated haemoglobin (HbA1c) serving as a predictive marker. However, measuring preoperative HbA1c is not routine, and there is no established threshold for deferring elective surgery. Preoperatively, emphasis should be placed on lowering the patient's HbA1c through optimized medical management and continuous glucose monitoring. Intraoperatively, continuous insulin infusion therapy is recommended alongside postoperative continuation for critically ill patients. Prompt resumption of the patient's routine medications post-surgery is also necessary.
Optimal glycemic control, both pre-, intra- and perioperatively, correlates with improved outcomes that are comparable to those without diabetes. Targeted efforts are warranted for patients with diabetes undergoing cardiac surgery to ensure long-term benefits for the patients and healthcare systems.
近年来,全球糖尿病患病率显著上升。因此,接受心脏手术的糖尿病患者数量有所增加。尽管存在国家和国际指南以改善糖尿病患者的手术结局,但围手术期糖尿病管理的优化仍不充分,导致这些患者的手术发病率和死亡率上升。本综述旨在评估糖尿病患者心脏手术后的结局,并评估加强术前和围手术期优化以及术后结局的策略。
对有关心脏手术患者糖尿病围手术期管理、糖尿病相关术后并发症以及用于优化结局的干预措施的文章进行了全面的文献检索。
提取并综合了主要发现。接受心脏手术的糖尿病患者围手术期并发症增加、院内死亡率更高且长期生存率较差。一个关键因素特别是血糖控制不佳,糖化血红蛋白(HbA1c)可作为预测指标。然而,术前测量HbA1c并非常规操作,且对于推迟择期手术没有既定的阈值。术前,应通过优化药物治疗和持续血糖监测来强调降低患者的HbA1c。术中,对于重症患者建议持续胰岛素输注治疗并在术后继续。术后及时恢复患者的常规用药也很有必要。
术前、术中和围手术期的最佳血糖控制与改善的结局相关,这些结局与非糖尿病患者相当。对于接受心脏手术的糖尿病患者,有必要进行有针对性的努力,以确保患者和医疗系统获得长期益处。