Sato Hisashi, Sakakura Kenichi, Jinnouchi Hiroyuki, Taniguchi Yousuke, Yamamoto Kei, Tsukui Takunori, Hatori Masashi, Kasahara Taku, Watanabe Yusuke, Ishibashi Shun, Seguchi Masaru, Fujita Hideo
Division of Cardiovascular Medicine, Saitama Medical Center, Jichi Medical University, 1-847 Amanuma, Omiya, Saitama City 330-8503, Japan.
J Clin Med. 2024 Nov 25;13(23):7136. doi: 10.3390/jcm13237136.
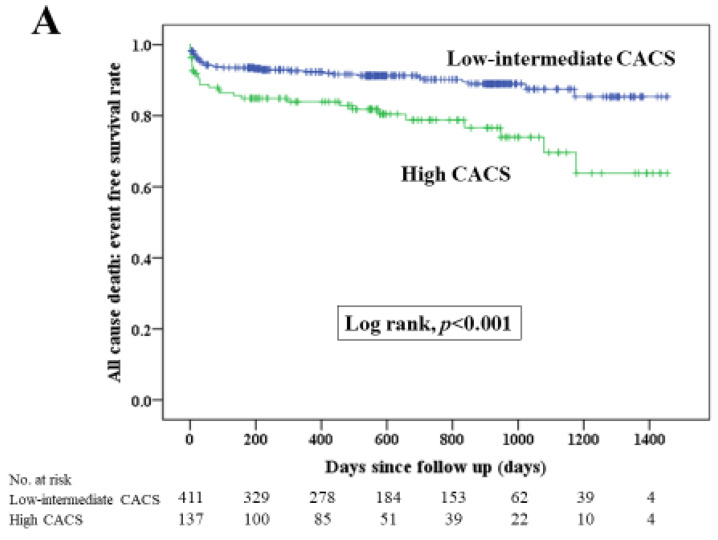
: It is essential to identify the risk factors for poor clinical outcomes in patients with acute myocardial infarction (AMI). The coronary artery calcium score (CACS) is gathering attention as a predictor for future cardiovascular events. This study aimed to (1) measure CACSs in patients with AMI by non-ECG-gated computed tomography (CT), (2) compare clinical outcomes between patients with a high CACS and a low-intermediate CACS and (3) to elucidate the association between high CACS and clinical outcomes. : We defined the high CACS group as the highest quantile of CACS (Q4) and defined the low-intermediate CACS group as the other quantiles of CACS (Q1-Q3). The primary endpoint was major adverse cardiovascular events (MACE), which were defined as the composite of all-cause death, re-admission for heart failure, non-fatal MI and target vessel revascularization. We included 548 patients with AMI who underwent non-ECG-gated CT and divided them into the high CACS group (CACS ≥ 5346.5, = 137) and the low-intermediate CACS group (CACS ≤ 5329.3, = 411). : During the median follow-up duration of 535 days, 150 MACE were observed. The Kaplan-Meier curves showed that MACE occurred more frequently in the high CACS group than in the low-intermediate CACS group ( < 0.001). Multivariable Cox hazard analysis revealed that a high CACS was significantly associated with MACE (hazard ratio 1.597, 95% confidence interval 1.081-2.358, = 0.019) after controlling for multiple confounding factors. : Clinical outcomes were worse in AMI patients with a high CACS than in those with a low-intermediate CACS. A high CACS was significantly associated with MACE in multivariate analysis.
确定急性心肌梗死(AMI)患者临床预后不良的危险因素至关重要。冠状动脉钙化评分(CACS)作为未来心血管事件的预测指标正受到关注。本研究旨在:(1)通过非心电图门控计算机断层扫描(CT)测量AMI患者的CACS;(2)比较高CACS患者和低-中CACS患者的临床预后;(3)阐明高CACS与临床预后之间的关联。我们将高CACS组定义为CACS的最高四分位数(Q4),将低-中CACS组定义为CACS的其他四分位数(Q1-Q3)。主要终点是主要不良心血管事件(MACE),其定义为全因死亡、因心力衰竭再次入院、非致命性心肌梗死和靶血管血运重建的综合结果。我们纳入了548例接受非心电图门控CT的AMI患者,并将他们分为高CACS组(CACS≥5346.5,n = 137)和低-中CACS组(CACS≤5329.3,n = 411)。在中位随访期535天期间,观察到150例MACE。Kaplan-Meier曲线显示,高CACS组MACE的发生频率高于低-中CACS组(P<0.001)。多变量Cox风险分析显示,在控制多个混杂因素后,高CACS与MACE显著相关(风险比1.597,95%置信区间1.081-2.358,P = 0.019)。高CACS的AMI患者临床预后比低-中CACS患者更差。在多变量分析中,高CACS与MACE显著相关。