Aldrich Luke, Ispoglou Theocharis, Prokopidis Konstantinos, Alqallaf Jasem, Wilson Oliver, Stavropoulos-Kalinoglou Antonis
Carnegie School of Sport, Leeds Beckett University, Headingley Campus, Leeds, UK.
Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, UK.
J Cachexia Sarcopenia Muscle. 2025 Feb;16(1):e13662. doi: 10.1002/jcsm.13662. Epub 2024 Dec 17.
Acute sarcopenia is sarcopenia lasting less than 6 months, typically following acute illness or injury. It may impact patient recovery and quality of life, advancing to chronic sarcopenia. However, its development and assessment remain poorly understood, particularly during hospitalisation. This systematic review aimed to elucidate the incidence of acute sarcopenia and examine changes in muscle parameters during hospitalisation.
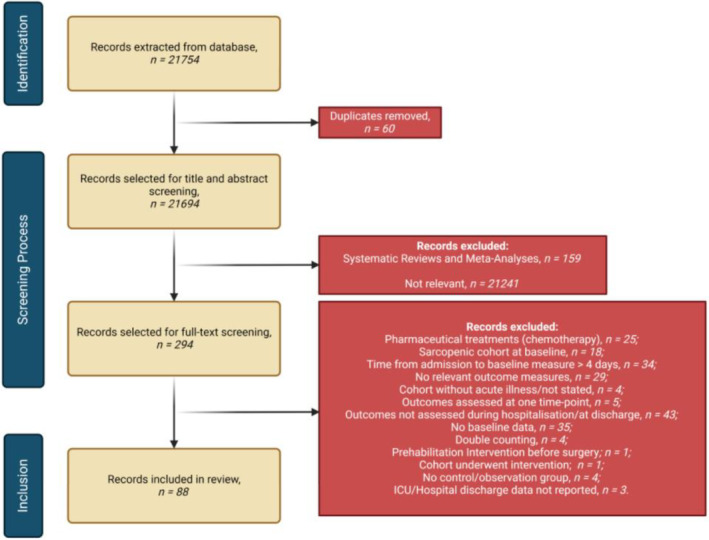
Eighty-eight papers were included in the narrative synthesis; 33 provided data for meta-analyses on the effects of hospitalisation on handgrip strength (HGS), rectus femoris cross-sectional area (RFCSA) and various muscle function tests. Meta-regressions were performed for length of hospital stay (LoS) and age for all meta-analyses; sex was also considered for HGS.
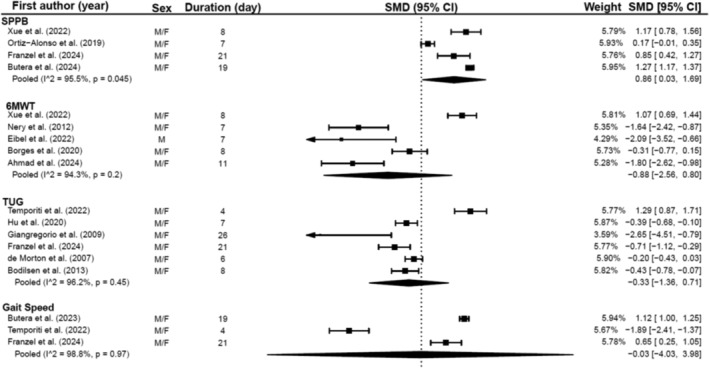
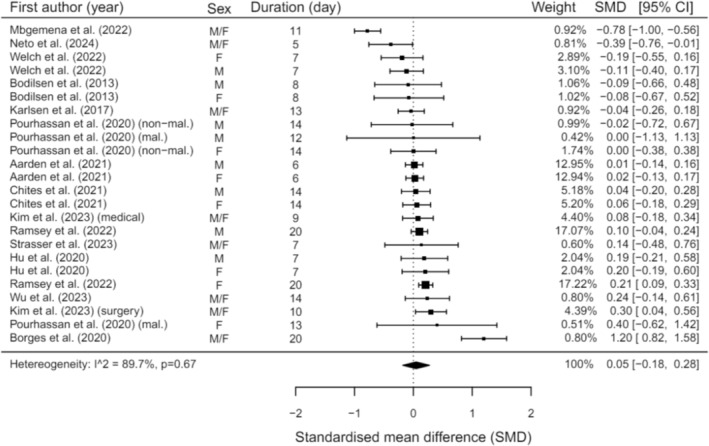
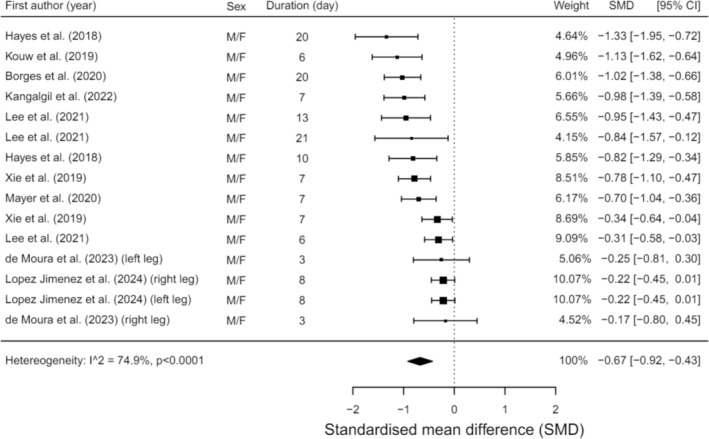
Acute sarcopenia development was assessed in four studies with a pooled incidence of 18% during hospitalisation. Incidence was highest among trauma patients in intensive care (59%), whereas it was lower among medical and surgical patients (15%-20%). Time of development ranged from 4 to 44 days. HGS remained stable during hospitalisation (SMD = 0.05, 95% CI = -0.18:0.28, p = 0.67) as did knee extensor strength. LoS affected HGS performance (θ = 0.04, 95% CI = 0.001:0.09, p = 0.045) but age (p = 0.903) and sex (p = 0.434) did not. RFCSA, reduced by 16.5% over 3-21 days (SMD = -0.67, 95% CI = -0.92:-0.43, p < 0.001); LoS or time between scans did significantly predict the reduction (θ = -0.04, 95% CI = -0.077:-0.011, p = 0.012). Indices of muscle quality also reduced. Muscle function improved when assessed by the short physical performance battery (SMD = 0.86, 95% CI = 0.03:1.69, p = 0.046); there was no change in 6-min walk (p = 0.22), timed up-and-go (p = 0.46) or gait speed tests (p = 0.98). The only significant predictor of timed up-and-go performance was age (θ = -0.11, 95% CI = -0.018:-0.005, p = 0.009).
Assessment and understanding of acute sarcopenia in clinical settings are limited. Incidence varies between clinical conditions, and muscle parameters are affected differently. HGS and muscle function tests may not be sensitive enough to identify acute changes during hospitalisation. Currently, muscle health deterioration may be underdiagnosed impacting recovery, quality of life and overall health following hospitalisation. Further evaluation is necessary to determine the suitability of existing diagnostic criteria of acute sarcopenia. Muscle mass and quality indices might need to become the primary determinants for muscle health assessment in hospitalised populations.
急性肌肉减少症是指持续时间少于6个月的肌肉减少症,通常发生在急性疾病或损伤之后。它可能会影响患者的康复和生活质量,并发展为慢性肌肉减少症。然而,其发展和评估仍知之甚少,尤其是在住院期间。本系统评价旨在阐明急性肌肉减少症的发生率,并研究住院期间肌肉参数的变化。
88篇论文纳入叙述性综合分析;33篇提供了关于住院对手握力(HGS)、股直肌横截面积(RFCSA)和各种肌肉功能测试影响的荟萃分析数据。对所有荟萃分析的住院时间(LoS)和年龄进行了荟萃回归分析;对手握力分析还考虑了性别因素。
四项研究评估了急性肌肉减少症的发展情况,住院期间合并发生率为18%。重症监护病房的创伤患者发生率最高(59%),而在内科和外科患者中发生率较低(15%-20%)。发展时间为4至44天。住院期间握力保持稳定(标准化均数差[SMD]=0.05,95%置信区间[CI]=-0.18:0.28,p=0.67),膝关节伸肌力量也是如此。住院时间影响握力表现(θ=0.04,95%CI=0.001:0.09,p=0.045),但年龄(p=0.903)和性别(p=0.434)不影响。股直肌横截面积在3至21天内减少了16.5%(SMD=-0.67,95%CI=-0.92:-0.43,p<0.001);住院时间或两次扫描之间的时间确实能显著预测这种减少(θ=-0.04,95%CI=-0.077:-0.011,p=0.012)。肌肉质量指标也有所下降。通过简短体能测试评估时,肌肉功能有所改善(SMD=0.86,95%CI=0.03:1.69,p=0.046);6分钟步行试验(p=0.22)、计时起立行走试验(p=0.46)或步态速度测试(p=0.98)没有变化。计时起立行走表现的唯一显著预测因素是年龄(θ=-0.11,95%CI=-0.018:-0.005,p=0.009)。
临床环境中对急性肌肉减少症的评估和理解有限。发生率因临床情况而异,肌肉参数受到的影响也不同。握力和肌肉功能测试可能不够敏感,无法识别住院期间的急性变化。目前,肌肉健康恶化可能未得到充分诊断,影响住院后的康复、生活质量和整体健康。需要进一步评估以确定急性肌肉减少症现有诊断标准的适用性。肌肉质量和质量指标可能需要成为住院人群肌肉健康评估的主要决定因素。