Song Jiyoung, Chae Kum Ju, Lee Jong Eun, Yanagawa Masahiro, Chung Jonathan H, Lynch David A, Jang Myoung-Jin, Goo Jin Mo, Yoon Soon Ho
Department of Radiology, Seoul National University Hospital, Seoul National College of Medicine, Seoul, Korea.
Department of Radiology, Jeonbuk National University Hospital, Jeonju, Korea.
Eur Radiol. 2025 Jun;35(6):3021-3029. doi: 10.1007/s00330-024-11259-5. Epub 2024 Dec 18.
We investigated whether supine chest CT alone suffices for diagnosing ILAs, thereby reducing the need for prone chest CT.
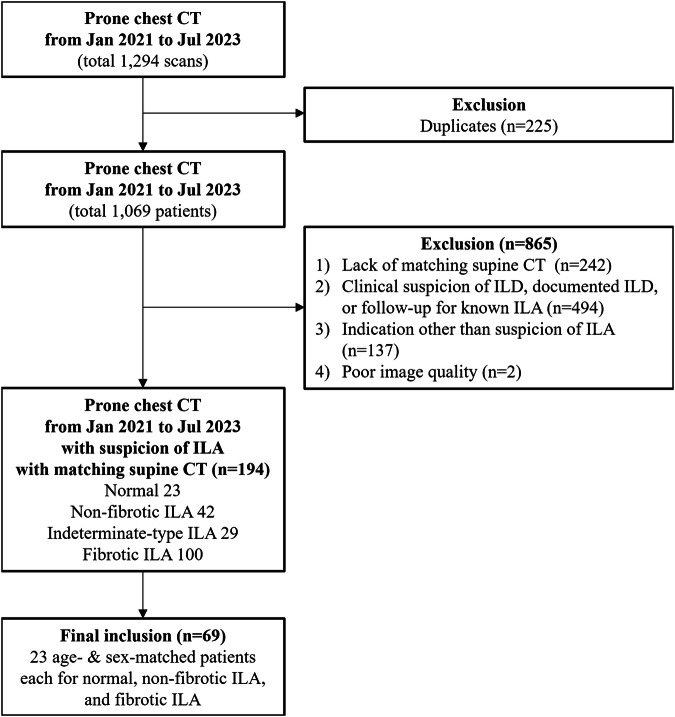
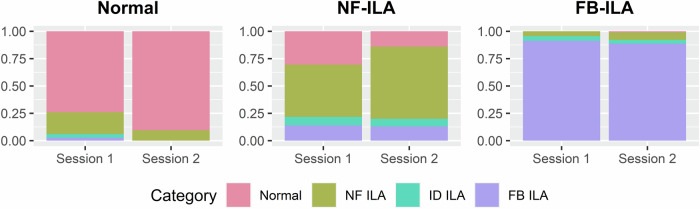
Patients who underwent prone chest CT for suspected ILAs from January 2021 to July 2023, with matching supine CT within 1 year, were retrospectively evaluated. Five multinational thoracic radiologists independently rated ILA suspicion and fibrosis scores (1 to 5-point) and ILA extent (1-100%) using supine CT first, then combined supine-prone CT after a 1-month washout. We categorized ILA suspicion and fibrosis scores into four diagnostic groups; normal, non-fibrotic, indeterminate-type, and fibrotic ILAs. The areas under the receiver operating characteristic curve (AUCs) of ILA suspicion scores, inter-reader agreement on diagnostic categories, and intra-reader/inter-reader reliability for ILA extent were evaluated.
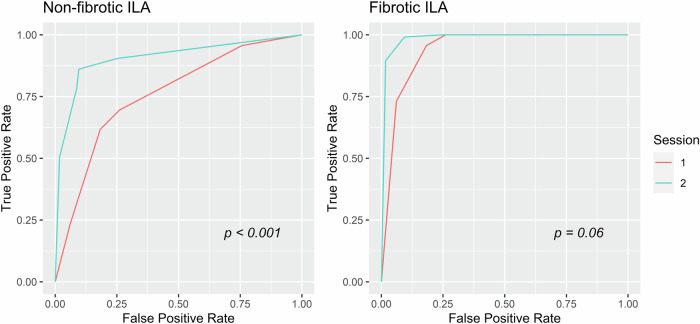
This study included 69 patients (mean age 67.2 ± 7.2 years; 36 women), with 23 age- and sex-matched patients in each group: normal, non-fibrotic ILAs, and fibrotic ILAs. The pooled AUC for ILA suspicion and inter-reader agreement on diagnostic categories improved for non-fibrotic ILAs with prone CT (AUC 0.76 to 0.92, p < 0.001; Fleiss kappa 0.25 to 0.51, p = 0.004), but not for fibrotic ILAs (AUC 0.94 to 0.99, p = 0.06; Fleiss kappa 0.63 to 0.72, p = 0.08). ILA extent was 1-2% smaller with prone CT for both ILA types (p < 0.001).
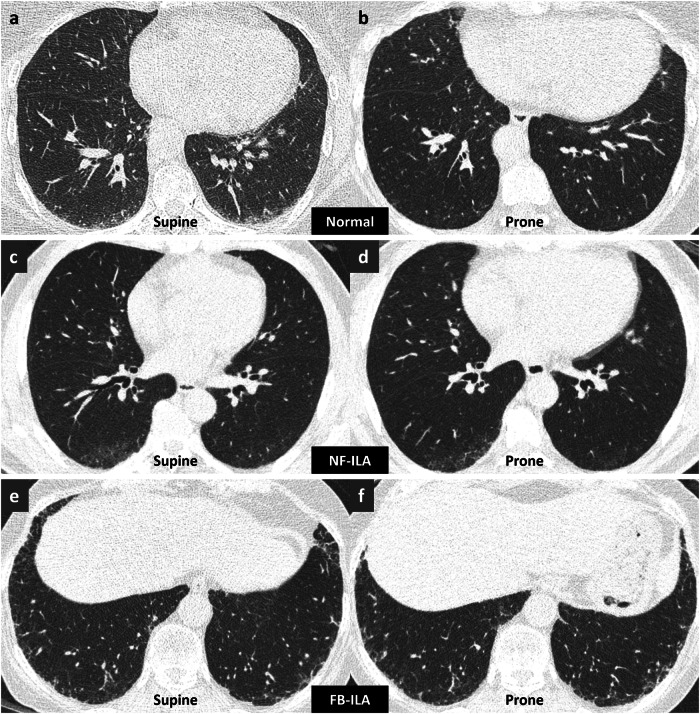
For fibrotic ILAs, supine CT alone exhibited substantial diagnostic accuracy and inter-reader agreement, while the diagnosis of non-fibrotic ILAs benefited from adding prone CT. Supine CT alone slightly overestimated extent regardless of ILA type.
Question Prone CT is recommended when interstitial lung abnormalities (ILAs) are suspected on supine CT, but its benefits remain underexplored. Findings Supine CT alone sufficed for diagnosing fibrotic ILAs, while prone CT improved non-fibrotic ILA diagnosis and reduced extent overestimation for both types. Clinical relevance Omitting prone CT reduces extra time, space, and radiation exposure without compromising the diagnosis of fibrotic ILAs, which have higher rates of progression and mortality risks, enhancing patient comfort and simplifying patient management.
我们研究了仅仰卧位胸部CT是否足以诊断特发性间质性肺炎(ILA),从而减少对俯卧位胸部CT的需求。
回顾性评估2021年1月至2023年7月因疑似ILA接受俯卧位胸部CT检查且在1年内有匹配仰卧位CT的患者。五名跨国胸放射科医生首先使用仰卧位CT独立对ILA怀疑度和纤维化评分(1至5分)以及ILA范围(1 - 100%)进行评分,然后在1个月洗脱期后使用仰卧位与俯卧位联合CT进行评分。我们将ILA怀疑度和纤维化评分分为四个诊断组:正常、非纤维化、不确定型和纤维化ILA。评估ILA怀疑度评分的受试者工作特征曲线下面积(AUC)、诊断类别上的阅片者间一致性以及ILA范围的阅片者内/阅片者间可靠性。
本研究纳入69例患者(平均年龄67.2±7.2岁;36例女性),每组有23例年龄和性别匹配的患者:正常、非纤维化ILA和纤维化ILA。对于非纤维化ILA,俯卧位CT使ILA怀疑度的合并AUC和诊断类别上的阅片者间一致性得到改善(AUC从0.76提高到0.92,p<0.001;Fleiss卡方从0.25提高到0.51,p = 0.004),但对于纤维化ILA未改善(AUC从0.94到0.99,p = 0.06;Fleiss卡方从0.63到0.72,p = 0.08)。两种ILA类型在俯卧位CT下ILA范围均减小1 - 2%(p<0.001)。
对于纤维化ILA,仅仰卧位CT就具有较高的诊断准确性和阅片者间一致性,而非纤维化ILA的诊断受益于增加俯卧位CT。无论ILA类型如何,仅仰卧位CT都略微高估了范围。
问题当仰卧位CT怀疑有间质性肺异常(ILA)时推荐使用俯卧位CT,但其益处仍未得到充分探索。发现仅仰卧位CT足以诊断纤维化ILA,而俯卧位CT改善了非纤维化ILA的诊断并减少了两种类型的范围高估。临床意义省略俯卧位CT可减少额外的时间、空间和辐射暴露,同时不影响纤维化ILA的诊断,纤维化ILA具有更高的进展率和死亡风险,可提高患者舒适度并简化患者管理。